
By Katie Stoll, MS
Katie Stoll is a genetic counselor in Washington State. She graduated from the Brandeis University training program in 2003 and since that time has held positions in the areas of prenatal, pediatric and cancer genetics.
A couple of years ago we were just beginning to learn about a new prenatal testing technology termed Noninvasive Prenatal Diagnosis. It was soon relabeled as Noninvasive Prenatal Testing, and now the American College of Medical Genetics and Genomics recommends this be taken one step further by terming it Noninvasive Prenatal Screening (NIPS) to highlight the limitations of this new technology.
As currently reported by labs, NIPS presents new challenges for genetic counselors. Of particular importance is figuring out how to convey to patients and healthcare providers why relying on sensitivity and specificity alone may lead to misinterpreted results. In the absence of positive and negative predictive values there may be a tendency to assume that the high sensitivity and specificity reported with NIPS means that these tests are more powerful – more diagnostic – than they actually are.
It is imperative that we understand both what the terms mean and how they relate to a person’s likelihood of having a condition. Sensitivity measures the true positive rate – the proportion of actual positives which are correctly identified as such (e.g., the percentage of fetuses with Down syndrome (DS) who have a positive test result). Specificity measures the true negative rate – the proportion of actual negatives which are correctly identified as such (e.g., the percentage of fetuses who do not have Down syndrome who have a negative NIPS result for DS).
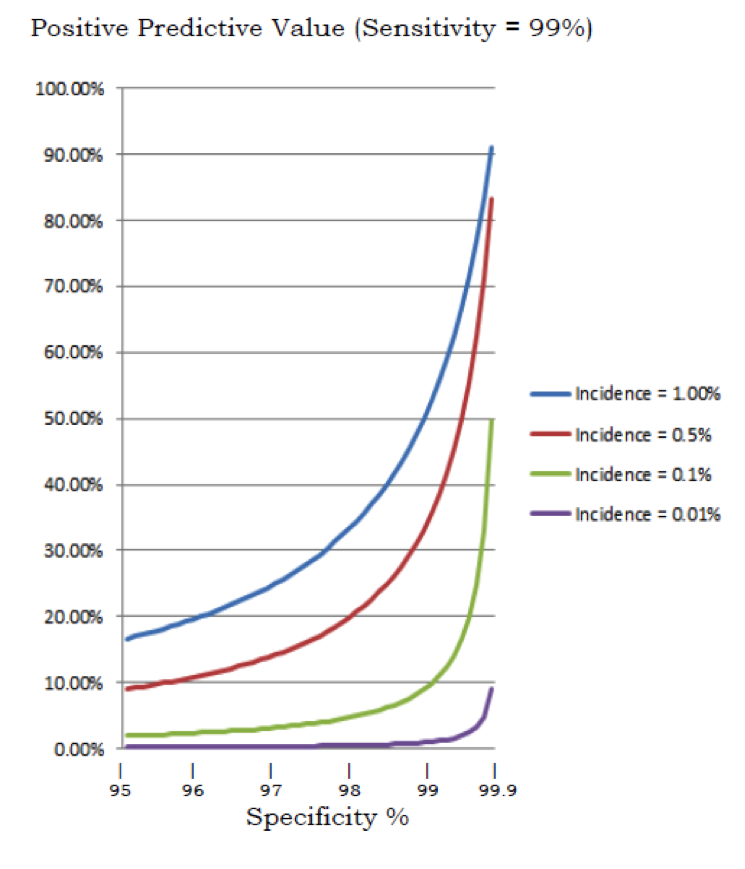
A test can have both a high sensitivity and specificity without being a good predictor of whether the condition is actually present. The likelihood that a positive test is a true positive result also depends on the incidence of the condition.
Genetic counselors are used to thinking about aneuploidy screening in terms of PPV, as this is generally the format for reporting maternal analyte screening such as Integrated , Quad screens, etc. Analyte screening takes into account the prior probability based on maternal age and provides a PPV as the end result. For instance, an analyte screen result may be reported as Positive with a 1 in 50 chance of Down syndrome. The PPV with analyte screening lets us know how many patients with a “positive” test will actually have a pregnancy affected with the condition and reporting results this way makes it clear that this is a screening test.
Can we apply the same interpretation to NIPS results? Some labs provide a “risk score” which appears similar to what we see with analyte screening, but I am told by the labs that the vast majority will be reported as either >99% chance or <.01% chance. Some labs do not report a risk score, instead giving essentially a positive or negative result. But does this mean that greater than 99% of women who receive a >99% or a positive result are actually carrying a fetus with Down syndrome or other chromosome condition?
Given that women 35 year and older are a population targeted for NIPS let me work out the expected NIPS results given the approximate sensitivities and specificities reported for a hypothetical population of 100,000 thirty-five-year old women (while I cannot tell you the specific number of women age 35 who give birth per year, CDC data suggests that for the past several years about 400,000 – 500,000 women in the age 35-39 have given birth each year in the United States – so 100,00 births annually by 35-year-old mothers is probably in the ball park of the national trend.
The performance data vary significantly from lab to lab – for the purpose of this illustration, I am using sensitivity and specificity in the range of what has been reported. The data below are based on the chance of Trisomy 21, 18 and 13 at the time of amniocentesis for a woman 35 at time of EDD1.
|
Down Syndrome |
Trisomy 18 |
Trisomy 13 |
|
| Incidence |
1/250 |
1 / 2000 |
1 / 5000 |
| Affected Fetuses |
400 |
50 |
20 |
| Sensitivity |
99.5% |
98.0% |
90.0% |
| Specificity |
99.9% |
99.6% |
99.8% |
| Total test positives |
498 |
449 |
218 |
| True test positives |
398 |
49 |
18 |
| False positives |
100 |
400 |
200 |
| Positive Predictive Value |
80% |
11% |
8% |
If we add all of the positive results together in a population of 100,000 thirty-five-year old women we see that 1165 (1.2%) have positive test results for Trisomy 21, Trisomy 18 or Trisomy 13. Note, though, that only 465 of these results will be true positives. This indicates that the majority of the time (greater than 60% using these statistics), a positive result on NIPS for a 35-year-old woman will be a false positive – and this doesn’t even include calculations for sex chromosome aneuploidy which some NIPS labs also screen for.
Notably, the negative predictive value for NIPS is very high indicating that a negative test result is a true negative >99% of the time. But how do we reconcile that for many women, the chance of a false positive with NIPS may be higher than the chance of a true positive result when that seems to be contradicted by way the labs are reporting the results?
In trying to explain the chance of a false positive result to patients with a “positive” test report in hand, I have found that I am met with disbelief. I can understand why – if a test says there is a>99% chance of Down syndrome and the lab says the test has >99% sensitivity and >99% specificity, how could this test be wrong?
While genetic counselors understand the limitations, the reporting practices of the labs place us in a position in which we have to work hard to convince our patients that NIPS is only a screening test.
Currently four labs offer NIPS in the U.S. and all have different strengths and weaknesses in their reporting practices. All could be improved by making the limitations of this technology more obvious. In some cases the language used in the reports gives the appearance that NIPS is diagnostic. For example, one company’s report suggests that the healthcare provider should advise for “additional diagnostic testing”. The labs vary in whether the need for genetic counseling following a positive result is recommended. Additionally there is variability in the transparency of how the performance data are derived.
Given that the performance statistics vary significantly, we need to be sure to take these details into account when considering PPV. I encourage genetic counselors and other healthcare providers to critically look at how the performance data are derived. The sample sizes on which these numbers are based are often quite small and the confidence intervals can be broad. I was surprised to see in the fine print of one report that the performance data “excludes cases with evidence of fetal and/or placental mosaicism.” Given that mosaicism is a known cause of false positive results and because mosaicism cannot be definitively determined through NIPS, it doesn’t seem accurate that these cases should be excluded from calculations of test performance.
The pitfalls of interpreting NIPS results is a challenge we need to address because NIPS is increasingly taking place without the involvement of genetic counselors in pretest or post-test counseling. There is real concern that patients are making pregnancy decisions based on screening tests with the misunderstanding that NIPS is diagnostic.
I write this as call to the NIPS labs to change their reporting practices to better emphasize the screening nature of this technology. Providing some positive predictive value estimates would be tremendously helpful as we try to make sense of NIPS results for our patients. While it may be difficult to provide individualized risk assessment, a general table of how prior probability impacts individual test performance would be beneficial for interpretation. Furthermore, eliminating language from the reports that suggests these tests are diagnostic and giving more transparency to ways in which performance data are calculated would also be welcome changes.
As genetic counselors, we strive to ensure informed decision-making for the clients we see. Key to informed decision-making is an understanding of the limitations of this evolving technology. As fellow patient advocates, I hope the genetic counseling community will join me in requesting increased accountability and responsible reporting on the part of the labs regarding NIPS.
I would like to acknowledge Evan Stoll, retired GAO data analyst for his contributions to this piece.
Please Note: Authors who contribute to The DNA Exchange cannot offer medical advice. Many commenters have raised interesting and thoughtful questions about NIPS. If you have undergone NIPS and have questions, you should meet with a certified genetic counselor. To locate a genetic counselor, go to the Find A Genetic Counselor section of the website of The National Society of Genetic Counselors.
- Hook EB. Prevalence, risks and recurrence. In: Brock DJH, Rodeck CH, Ferguson-Smith MA, editors. Prenatal Diagnosis and Screening. Edinburgh: Churchill Livingston, 1992.








{kind=link}
{kind=link}