As the genetic counseling world knows all too well, the New York Times recently published a story about prenatal cfDNA screening for chromosomal microdeletion syndromes. The gist of the article is that screening for microdeletions has a high number of false positives that produce significant patient anxiety and, in a very small number of cases, patients have elected to terminate a pregnancy before confirmatory diagnostic testing. The Times piece generated 1100+ comments on its site, including many from genetic counselors and physicians, not to mention vitriolic sturm und drang on various social media.
Clearly the article touched a collective genetic counselor nerve — a lot of the reaction has been more reflexive than reflective. Which is kind of surprising, considering that cfDNA for microdeletions is a so-so screen for a handful of rare conditions that genetic counselors have not widely agreed should be included on these tests.
Most of the criticism centered on the article not always making a clear and consistent technical distinction between a screaming test, er, uh, I mean, a screening test (which cfNDA is) and a diagnostic test (which cfDNA is not). This confusion has been an ongoing problem since the early to mid-1980s when AFP screening for neural tube defects — and maternal anxiety over testing — was first working its way into clinical practice (I remember one of my patients back then referring to AFP as “alpha-fucking protein”). Forty years later, and the anxiety and misunderstanding has not improved much.
Some of those criticisms are fair, particularly when the article describes cfDNA results as being “wrong” or “inaccurate.” To the specialist, the term false positive has a very specific definition,* and hence the source of the reaction to the article. But from a semantics standpoint, doesn’t the word false in false positive imply wrong? You can also think of calling a result “wrong” as an example of the tried and true counseling strategy of reframing, i.e. “Well, Jane, your test result actually says that there is more than an 80-90% chance your baby does not have a microdeletion.”
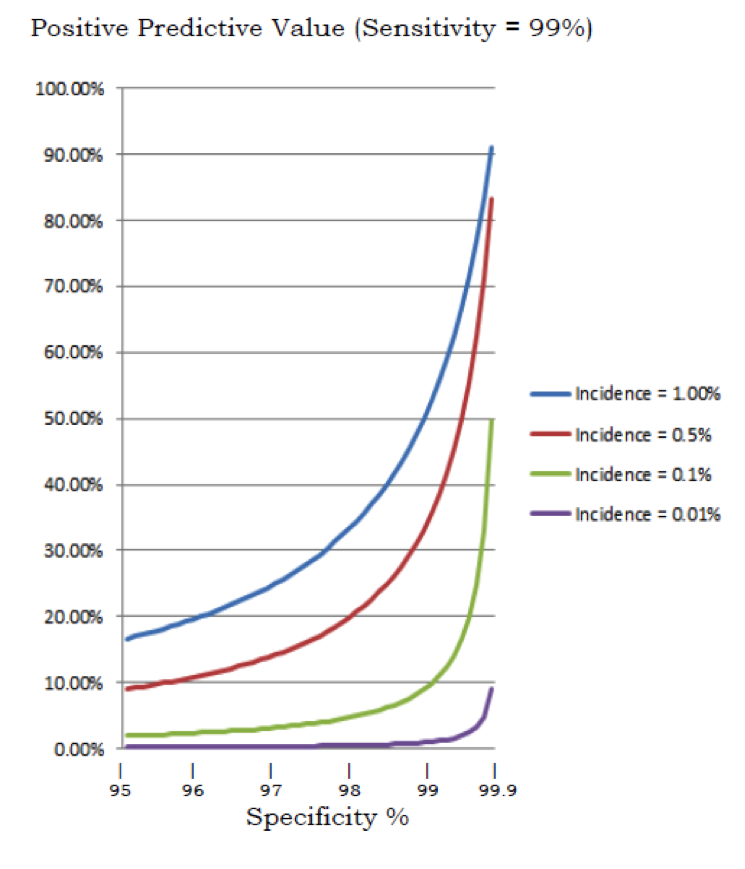
In my opinion the article otherwise does a decent job of highlighting the statistical complexities of cfDNA. The accompanying Figures are helpful in explaining what is essentially the positive predictive value of the tests. In fact, I think the graphics are better than the explanations and graphics on many of the testing laboratories’ websites. Many of these websites are even guiltier of muddling the differences between screening and diagnostic tests, and labs really should know better. It’s no wonder that patients might be confused and anxious when they read that a test is “highly accurate,” “an alternative to amniocentesis or CVS,” and can be assured of a “healthy baby” when results are normal. To be fair, some of the websites also address the distinctions between screening tests and diagnostic tests, but only if you click down into the rabbit warren of information.
I think most of the criticism by genetic counselors glosses over more important and fundamental questions that should be the focus of critiques of prenatal testing and our reaction to the Times piece (here I am defining prenatal testing as including screening and diagnosis). These critical questions include:
• Should we test for any condition prenatally? This is an ethically and for some a religiously complex question but it underlies all of the subsequent questions.
• If there is broad agreement that prenatal testing should be available, then what is its purpose? Realistically, with a few exceptions, is there any purpose beyond selective termination? While termination is an important option and benefit of the test for some, it’s not a course of action that all parents will choose. Some parents might decide to have prenatal testing for “preparation” but as I have argued elsewhere there is minimal data saying one way or another whether prenatal knowledge of a condition helps babies or their families, medically, emotionally, or developmentally (thought at least one study is beginning to address this shortcoming). If patients are going to be put through the emotional ringer of prenatal testing, we should be able to provide solid data on whether prenatal knowledge of a condition provides benefits in addition to the option of termination.
• What criteria should be used in determining which conditions should be subject to prenatal testing? Even if every genetic condition could be detected prenatally (and we might actually get close to that point one day), it wouldn’t make sense to test for many of them. Clinically rational and ethically acceptable criteria need to be developed to guide the selection of conditions to consider for prenatal testing.
• Who decides which conditions are screen-worthy? As Ilana Löwy and others have noted, commercial labs often spearhead this choice but decisions are reinforced and supported by the medical and genetics communities that order the testing. If no one ordered a test, labs wouldn’t offer it. As Liza Minelli, Joel Grey, and Scarface remind us, money makes the world go around. Are we screening for some conditions primarily because we can screen for them and labs offer it? What about input from patients, the public, multiple medical specialties, ethicists, social scientists, people with disabilities, and others?
• Is widespread screening for rare conditions the best use of laboratory and genetic counseling resources? Follow up of screen positive results consumes a significant amount of genetic counselor time and energy, to say nothing of patients’ anxiety and health care costs. Should these resources be focused on more pressing conditions?
• Many jobs in the genetics sector — labs and clinical providers — are dependent on the existence of genetic testing. Labs make their living off of testing but so do many genetic counselors working in clinics. While genetic counselors are not trying to push testing on patients, many genetic counseling jobs depend on the availability of genetic testing, either helping patients decide whether to have a test or explaining results to them once the testing has been completed. For better and worse, the genetic counseling profession has intimately identified itself with genetic testing. Clinics would employ far fewer prenatal, cancer, cardiogenetics, and other specialty genetic counseling jobs if there were not so many genetic tests. Think about how many clinical positions would evaporate if prenatal testing — or, really, almost any genetic testing — disappeared tomorrow. Some jobs would remain, for sure. But the demand for genetic counseling would likely drop off significantly if fewer tests were available. How much does this conflict of interest influence genetic counselors’ attitudes toward, and willingness to adopt, genetic tests, and how much does it subtly and subconsciously influence some of the strong reaction to the Times article?
• First and foremost, a patient’s decision to undergo — or not — prenatal testing should be preceded by a soul-searching exploration with partners and care providers about what parents want out of their children and addressing parental fears of disability, along with ethical and spiritual reflection. The decision requires more emotional expertise than numerical expertise. Should we be offering tests to all pregnant women that require them to master abstruse statistical knowledge in order to decide about whether to pursue testing? Even in a (unrealistic) world where all pregnant patients meet with a genetic counselor prior to testing and everything was explained in excruciating detail, many patients will misinterpret, forget, and misunderstand most of the technical information about false positives, false negatives, and distinctions between diagnostic tests and screening tests. What is the best way for patients to make medically and emotionally informed decisions? Laboratory website are less than ideal sources of information. Websites are essentially marketing tools, and marketing is antithetical to nondirectiveness. Chatbots alone don’t cut it for this purpose, although they could have an ancillary role.
• What message does it send to people with disabilities, their families, and their advocates if we continually add, seemingly willy-nilly, more and more genetic conditions to the prenatal testing list, especially, as I noted above, if they obtain no tangible benefit from testing? More testing readily begets further routinization of testing. And when you start testing lots of pregnancies for lots of conditions, you start creeping further into eugenic territory.
There are no easy solutions to any of these questions. Some may very well prove to be unanswerable and some parties will remain dissatisfied if we do manage to come up with some answers. It will involve vigorous and at times contentious debates among multiple viewpoints, and lots of people convinced that they are so damned right and why the hell can’t everybody else see that? But that doesn’t mean we shouldn’t be taking on the challenge. We may wind up with less than perfect answers, but they will be better than what we are doing now. The practice of genetic counseling demands it and patients deserve no less.
__________________________________________________________________
*- Another source of confusion here is the distinction between the false positive rate and a false positive result. The false positive rate is the number of pregnancies that do not have a condition but test positive. Thus, a lab can accurately claim that cfDNA for microdeletions has a false positive rate below 1%. You can see why a patient with a positive result might misinterpret that to mean there is over a 99% chance that her baby does indeed have a microdeletion. On the other hand, a false positive result is one specific patient’s test result which incorrectly indicates that a condition is present. Thus a patient who has a positive microdeletion result has an 80-90% chance that her baby does not have a microdeletion. Lord have mercy! You can see why pregnant patients might be confused. Then try to sort through all that while experiencing the joys of hyperemesis, or if you are a non-English speaking immigrant from a village in Central America working through an interpreter, or if you are also trying to figure out at about the same time the meaning of your rubella result, your HIV status, your nuchal thickness scan, and the results of your carrier testing.