Jon Weil is an independent scholar focusing on psychosocial aspects of genetic counseling and on international genetic counseling defined broadly and deeply. This post is based on a section in his chapter 6 of Grubs et al. The Oxford Handbook of Genetic Counseling, in an effort to disseminate the ideas more broadly and stimulate discussion. That section, in turn, is based on his chapter 7 in Leroy et al. Genetic Counseling Practice: Advanced Concepts and Skills as well as the work of many other clinicians and scholars.
Patient resistance in genetic counseling takes many forms. When overt it may manifest, for example, as questioning the genetic counselor’s training and competence or refusing to continue the consultation. When subtle it may involve behaviors such as denying aspects of family history or arriving slightly late for an appointment. Intermediate examples include repeatedly changing the subject to an apparently irrelevant topic or inappropriate humor. It almost always involves an element of self-protection and/or protection of others, and most such behaviors can also be thought of as psychological defenses.
Overt resistance is clearly problematic for the genetic counselor. It may evoke a variety of responses such as frustration, concern about one’s professional competence, and a loss or reduction of empathy. Intermediate or subtle resistance may or may not require an adjustment in the genetic counselor’s responses. But whatever the response, patient resistance is often perceived as an impediment to the flow of the session and to pursuing the genetic counselor’s mandated and desired agenda.
Patent resistance has a central role in psychodynamically-oriented psychotherapy. The iterative, often multi-session process of identifying, acknowledging, exploring and at least partially addressing the underlying issues that led to the resistance is a major path toward resolving emotional issues. This is not possible or appropriate in genetic counseling. However, as genetic counselors are well aware, listening carefully and responding effectively is appropriate and often necessary. Thus, I wish to propose a different way to think about patient resistance:
Patient resistance is critically important, often at least partially non-verbal communication that, if properly attended to, can be immensely helpful in achieving the goals of the genetic counseling session.
I suggest that the reader’s introspection, like my own, will make this clear. When my cardiologist says, “You need to start taking your cardio-walk four times a week instead of three”, my immediate, self-protective response is, “I can’t; that is too much”. However, it is not the details of this interaction that are important. It is the fact that, at that moment, this isthe most important, actually the only, issue on my mind. That is why it is so productive to interpret patient resistance as communication!
What are the implications of this reframing?
First and foremost, it puts the genetic counselor in direct, often at least partially non-verbal, contact with the fear, anxiety, confusion, desire to protect self and family, or other emotion or cognition that is consuming the patient at that moment. The evolving response that is crafted can then help both genetic counselor and patient address this critical issue. For example:
“I have been telling you about how this test works and what the results might be. But I didn’t realize until now that your primary concern is how the result might affect the rest of your family.”
(This is in part non-verbal because, behind what is said is the implicit message: I hear what you have been trying to tell me.)
Second, it may allow a more empathic, deeply understood response to the patient that potentially deepens the conversation in the remainder of the session and beyond.
Third, it may influence countertransference that the genetic counselor is experiencing. It will not necessarily reduce it. More direct contact with the patient’s fear, anxiety or hopelessness may increase the genetic counselor’s own concerns about working with the patient or resonate with her prior experiences. However, as already indicated, it may also help convert more difficult feelings into empathy and understanding, thus easing the burden of the interaction. Whatever the circumstances, as I have previously argued in chapter 8 of Leroy et al. Genetic Counseling Practice: Advanced Concepts and Skills, aligning the genetic counselor’s countertransference to more accurately reflect the patient’s concerns should improve its value as a guide to further interventions.
To conclude, perceiving patient resistance as communication, whatever its form and intensity, provides a key to identifying and responding to the most salient issue of the moment, thus advancing the conversation productively.
Jon Weil was Director of the Program in Genetic Counseling, University of California Berkeley, from 1989 to 2001 and is the author of Psychosocial Genetic Counseling, Oxford University Press, 2000. He retired in 2001 but has remained professionally active. His current interests include the continuing development of psychosocial genetic counseling and promoting locally focused, patient-oriented international genetic counseling.
Robert Resta is a happily retired genetic counselor who has been a frequent contributor to the DNA Exchange since its inception in 2009.
Like a zombie, nondirective genetic counseling is a concept that refuses to die. It’s as old as genetic counseling itself and attempts to expose its shortcomings are just as old. But nondirectiveness refuses to go away. It keeps getting re-born in different guises – an antidote to eugenics or paradoxically a subtle form of eugenics, a variation on Dr. Carl Rogers’ patient-centered therapy, a philosophy underlying the educational model of genetic counseling, a natural corollary of patient autonomy, a basis for shared decision making, and a defense against engaging fully with the patient’s practical, emotional and medical needs and circumstances. Our impression is that in everyday practice most genetic counselors conceptualize nondirectiveness as some variation of “I shouldn’t tell the patient what to do,” even though there are times where you really should tell the patient what to do.
So, the whole point of therapy (not only for “borderline” patients but for all patients) is for the therapist to act as a container [bold in original]: they need to remain calm enough, and neutral enough in order to gracefully receive the projections, identify with them “just enough” so that they can understand them, contain them, then metabolize them, and then return them back to the patient in a more palatable and thinkable form. And this is a lot to ask of a person but that’s the job…
In the context of psychotherapy, the therapist and the therapy session endeavor to be a container – a safe, relatively neutral place for processing complex, emotionally charged, traumatic, or uncomfortable emotions, thoughts, or feelings. The therapist’s role is to nonjudgmentally absorb this psychic outpouring, help make emotional and cognitive sense of it, and then frame it and feed it back in a coherent and digestible form so the patient can have the wherewithal to cope with the issues at hand. This can help the psychological distress to be more effectively handled in the patient’s daily life outside the container.
In our view, this paradigm can be applied to genetic counseling, opening the conversation to some version of directiveness while maintaining respect for the primacy of the patient.
Here are some examples that illustrate how this might look in a genetic counseling session. In each scenario, the genetic counselor has carefully listened to the patient’s worries, anger, and anxiety, absorbed and framed them, and is providing feedback:
• You just told me that you are very worried about your ovarian cancer risk now that your BRCA1 test was positive and having had first-hand experience with ovarian cancer when you cared for your mother when she was dying of it. You are 50 years old. The strong medical recommendation in your situation, and one that I endorse, is that you should have your ovaries and fallopian tubes removed as soon as reasonably possible. Yet at the same time you are very reluctant to undergo the procedure, and you already canceled a surgical appointment. Let’s talk about why you canceled that appointment and what your fears and concerns about it are, beyond your immediate reason of having “a very busy schedule.” • From what you have been telling me, you are trying so hard to be a good parent and do your utmost to make sure your daughter is getting the best possible medical care. It also sounds like you have had less-than-ideal experiences with some medical professionals. But a whole genome test might give you and her care providers a better understanding of what is going on with your daughter – with her great smile that melts everyone’s hearts – and help guide her treatment. You have some very understandable concerns about the privacy of genetic testing when the analysis is performed by a large commercial lab. But the concrete advantages of the testing might outweigh the potential of violating her privacy at some point in the future. How do you weigh one against the other? • You have been reluctant to take your medication because you think that doctors don’t really know enough about the safety of it in pregnancy and you are in that developmentally sensitive period of early pregnancy. And you are right – we don’t have anywhere near as much data as we would like to have. But if your medical condition stays untreated, that would definitely pose a risk to the baby’s health and development. If you are not healthy, there’s a pretty good chance that will affect the baby in not good ways. This is a difficult decision but taking your medications I think ultimately is in the baby’s – and your – self-interest. How have you gone about making other decisions about how you care for yourself and your baby during this pregnancy?
But even with the best counseling skills, some patients make decisions that appear to be inconsistent with their own best interests, beliefs, or values. This does not necessarily represent a counseling failure. It can be very difficult to determine if a decision is “good” or “bad.” What looks like a good decision in the moment may in the long run prove to be a bad decision, and vice versa. Sometimes, too, patients are just not ready to make a decision and so they choose the easiest way out for the moment. And sometimes people just make bad decisions, accept the consequences, and move on with their lives.
Of course, no counselor is ever neutral. We are all embedded in personal, social, economic, historical, and cultural contexts that may be quite different than those of our patients. The result is that patients and genetic counselors can have very different frames of reference for perceiving and evaluating information. Those different frames of reference can color counseling sessions both overtly and subtly and throw a monkey wrench into the counseling works. But like Donald Winnicott’s concept of a Good Enough Parent, genetic counselors should strive to be neutral enough* to function as safe containers, whatever personal feelings they may harbor towards patients, their decisions, or their views. As Zavlis points out, this is no mean feat. It is all the more difficult to achieve in genetic counseling, which, for most patients, is a one or at most two-shot deal. It requires a healthy dose of personal and professional growth, along with a good understanding of the psychological meaning of patients’ words, choices, and actions. And it emphasizes the need for ongoing professional supervision and education throughout our careers.
Being appropriately directive in certain situations in genetic counseling demands wisdom, knowledge, self-awareness and a recognition of the ethical necessity to give our patients the full extent of our expertise. We may never vanquish the zombie. But we can move to a place from which to use our expertise fully – directional when appropriate without fear of being directive.
______________________________________________________________ * Yes, we recognize that “neutral enough” is more or less a contradiction in terms
In a recent thoughtful commentary in Genetics in Medicine and an ELSIhub Journal Club, Amicia Phillips, Maria Siermann, and colleagues critically examined the concept of actionability in the context of prenatal and newborn genomic screening. The authors conclude that actionability is poorly operationalized and call for “a need to develop a clear and nuanced understanding of actionability to ensure that screening policies are both ethical and effective.” I am not going to re-hash their ideas here, but some key considerations they raise include asking the questions Actionable how? Actionable when? Actionable for whom? Actionable at what level? I encourage you to read the article and view the ELSIhub Journal Club when the recording becomes available.
I have no insights or suggestions on how to develop a better understanding of actionability. I will leave that to folks smarter and more informed than me. But the article and webinar got me to thinking about the relationship between utility and actionability. Here I propose a model for thinking about these concepts and how they might be applied in genomic medicine. I recognize that both concepts are plagued by ambiguity. But for purposes of my model, utility is defined as the likelihood that a genomic/genetic test will, by prompting an intervention or other action, result in an improved outcome (a slight modification of the NCI definition). Going with the Phillips et al. paper, actionability is defined as “whether the information generated by screening leads to actions that may be undertaken” (to which I would add information generated by diagnostic testing too).
Utility typically includes two domains – Personal and Clinical Utility. In my model, I include a third domain that I call Public Health Utility. The types of actionability vary within each domain.
Personal Utility can be measured by the efficacy of actions that a person or family may take as a result of genomic/genetic testing that has the potential to improve their emotional, psychological, medical, and socioeconomic well-being. Using the recommendations of Kohler et al., these can be broadly categorized as affective, cognitive, behavioral, and social benefits. Some examples of actionability items include making reproductive decisions; choosing (or not) a medical course of action; joining a support group; accessing educational resources such as an appropriate educational plan for a child; applying for health and financial benefits such as Medicare and Social Security Disability Insurance in the US; participating in research about a specific genetic condition; and engaging in a psychotherapeutic relationship and other measures that can enhance emotional and psychological adaptation to a test result or genetic condition in the patient or within a family.
Clinical Utility can be assessed by the efficacy of actions that a clinician may take as a result of genomic/genetic testing that could improve the health outcomes of a particular patient or set of patients. These might include instituting specific screening modalities such as medical imaging as well as pharmaceutical, surgical, and other treatment and risk-reducing strategies, or suggesting alternative strategies. Actionability can also paradoxically include non-actions, such as discontinuing a treatment or recommending against a treatment or screening modality.
Public Health Utility can be assessed by the efficacy of actions taken by governmental and professional bodies based on genomic/genetic testing that may improve health outcomes on a population level. These actions might include allocating resources and finances, optimizing medical infrastructure, identifying research priorities, establishing clinical guidelines, and ensuring socially just and equitable access to genetic testing and subsequent recommended medical care and other health-related resources.
All three domains of utility feed into one another and are intertwined like a triple helix, so it can be difficult sometimes to separate them out. But the model* does provide a framework for evaluating utility and actionability. A test can be evaluated for its actionability in the different domains and weighed for the benefits and risks across domains. A test might provide little Clinical or Public Health Utility but still be justified if it provides significant Personal Utility. Or within a given domain, actionability may not provide enough utility to justify the test but if the benefit is moderate across all 3 domains the sum of the benefits may provide enough utility to justify the test. Or a test may have different actionability at different times of life and that too can be included in assessing utility.
Decisions about the utility of the actionability of genomic/genetic testing should be based on ethics, resource and financial availability, practicality, and statistical analysis, with input from patients, clinicians, the public, researchers, health policy analysts, and other stakeholders. Phillips et al. offer a much needed nudge in that direction. Of course, what counts as a benefit and how to weigh those benefits is no simple matter but that should not stop us from going through the process. Fear of imperfection should not be the enemy of the good.
Artificial Intelligence was not used to research or compose or edit this blogpost, nor was it used to generate the image.
_________________________________________________
Okay, let’s call it The Resta Model or The Resta Framework. Unless somebody else has already proposed this model and I didn’t realize it or it turns out be be a lousy model in the real world.
Things they do look awful c-c-cold/Why don’t you all f-fade away?/And don’t try to d-dig what we all s-s-say/Just talkin’ ’bout my g-g-generation – “My Generation” by Pete Townshend and The Who
The boast in the title of this piece is not aimed at the generation or two of genetic counselors who entered the field after I graduated from the UC Irvine genetic counseling program in 1983. Instead, it verbalizes the ethical conceit on the part of genetic counselors and medical geneticists in any given era that previous generations of geneticists always seem to have glaring ethical lapses. Yes sirree Bob, we learned our historical lessons from studying what they did wrong. We are good people with high ethical standards and would never say or do anything as bad as they did. Our moral compass is pointed to True Ethical North.
And so we create self-serving historical narratives that tell a tale of past sins and generational redemption.* Like Dante’s Divine Comedy, the genetic counseling narrative is a journey from Inferno (classical eugenics) to Purgatorio (post WW-II and the professionalization of medical genetics) to Paradiso (nowadays). Each step of the journey we strive to become better people and better genetic counselors, though the comedy may not be so divine. Think of me as your Virgil, and follow me on a journey through the history of genetic counseling and medical genetics.
Eugène Delacroix’s 1822 painting of Virgil guiding a fearful Dante across the River Styx, which is crowded with tortured souls at the entrance to Hell. As far as I am aware, there is no circle in Hell for geneticists. Yet. Source: https://en.wikipedia.org/wiki/The_Barque_of_Dante
Inferno
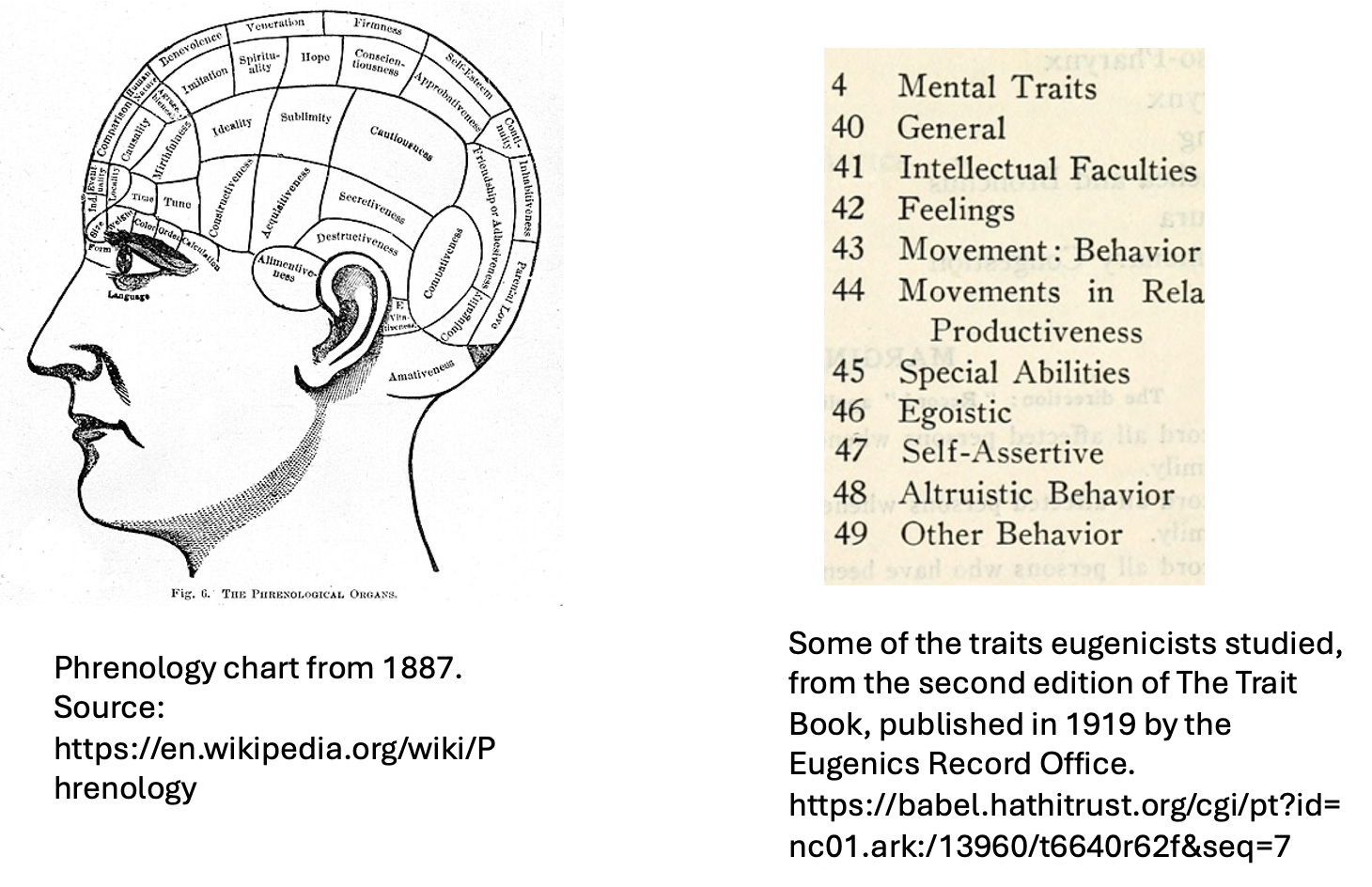
The scientific study of human genetics was conceived with the Original Sin of Eugenics on its soul (keeping up Dante’s religious imagery). For several decades into the 20th century, genetics and eugenics were more or less inseparable. Almost all major geneticists espoused eugenic ideology. And no, eugenics was not a pseudoscience; that is another conceit of the present passing judgment on the knowledge base of the past. In fact, eugenicists themselves dismissed its predictive forebear, phrenology, as a pseudoscience while heralding genetics as a true science of human traits and behavior. But to our 21st century perception, there is a slim difference between reading skulls and reading pedigrees.
A comparison of behavioral and personality traits studied by phrenologists and eugenicists.
Eugenicallly-minded geneticists were not stupid; many were brilliant scientists who had a very sophisticated understanding of genetics, the environment, and statistics, at least within the context of the times. Highly respected geneticists such as Karl Pearson, Herman Muller,Lancelot Hogben, Ronald A. Fisher, and Raymond Pearl criticized some of the less sophisticated eugenic applications of genetic knowledge but nonetheless remained staunch eugenicists. Heck, even Franz Boas, the anthropologist who is often cited as the ultimate anti-eugenicist, supported sterilization for reasons of “hereditary unfitness.” Boas, one of the most forceful critics of theories of racial superiority, also internalized some of the standard beliefs of the time about so-called primitive cultures. In 1897, he had the polar explorer Robert Peary essentially kidnap six Greenland Inuqhuit men, women, and children and bring them to the American Museum of Natural History in New York City so they could be studied as biological and anthropological specimens.**
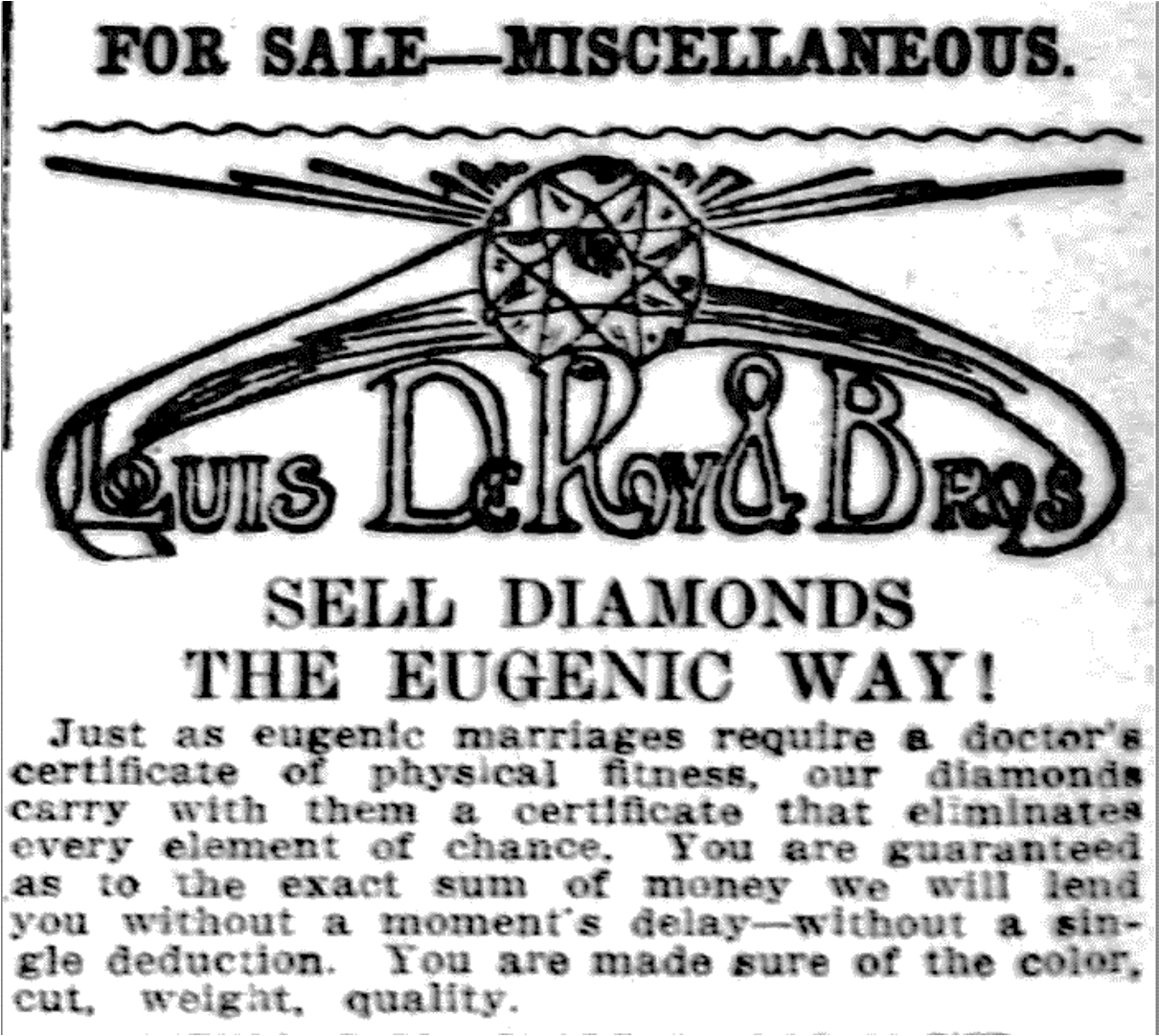
I am not trying to justify eugenic ideology or programs or serve as an apologist. There were many different versions of eugenics that arose around the globe and over time (and continue to do so). Each version was bad, but often bad in its own way. Eugenics was pervasive and cut across all economic and ethnic segments of society. It was taught in high schools and colleges, it appeared in advertisements for consumer products, and newspaper stories. Support of eugenics wasn’t universal but it sure was widespread.
Advertisment for a Pittsburgh jewelry store from the early 20th century, courtesy of Paul Lombardo.
The biases and beliefs of earlhy 20th century geneticists reflected some of the major social issues of their day – large scale immigration from non-Western European countries of people thought to be morally, intellectually, and physically inferior; the growth and increasing visibility of urban poverty with increasing urbanization along side an extremely wealthy upper class; the supposedly low IQ and poor health of the millions of soldiers who enlisted or were drafted to fight in the First World War (and English soldiers who fought in the Boer War). Geneticists from this period were products of these times who also simultaneously helped shape their era. It is also unsurprising that the vast majority of the early eugenicists were men at a time when men still felt that they had the right to make reproductive, economic, and other life decisions for women. It is easy to call out their moral shortcomings – bigotry, racism, smug moral superiority, ableism, classism, sexism, etc. Some eugenicists were truly evil and many inflicted all kinds of awful harm but for the most part they were a bunch of flawed human beings, just like we are. They were reacting to what they perceived to be threats to their way of life and to (White Western European-centric) civilization, and many thought eugenics was a way of helping eugenically inferior people.
Cover of the June, 1934 edition of the popular magazine Physical Culture, with an article by the eugenicist Albert Wiggam titled “Shall We Breed or Sterilize Defectives?” To my eyes, the magazine cover evokes the Sidney Sweeney ads that teased eugenics and eros to sell jeans. Source: Ball State University Digital Media Repository, https://dmr.bsu.edu/digital/collection/PhyCul/id/22511
Purgatorio
The next phase in the historical development of genetic counseling was the rise of medical genetics as a clinical and research discipline in the decades following the end of the Second World War, critically examined in Nathaniel Comfort’s classic book The Science of Human Perfection. The mytho-story often told – which, zombie-like, refuses die and that Comfort and other historians have long repudiated – is that the founding figures of medical genetics and genetic counseling specifically rejected eugenic ideology, in part driven by the horrific practices of Nazi Germany. Medical geneticists took great pains to distance themselves from the excesses of their eugenicist forebears and criticized eugenics for its ethical shortcomings and simplistic understanding of genetics. Indeed, in 1947 Sheldon Reed famously defined genetic counseling as “a kind of genetic social work without eugenic connotations.” But, at the same time, many geneticists maintained membership in the American Eugenics Society and espoused beliefs and genetic counseling principles that to 21st century sensibilities sounds an awful lot like eugenics disguised as “educated parental choice” (Reed joined the society in 1956 and remained a member through nearly 2 decades and a few name changes of the society).
Some of the major social issues of this period were the worry about over-population of the earth (largely in poorer, non-White countries) in the context of supposedly limited resources, the health and genetic effects of ionizing radiation from nuclear bomb testing and detonation sparked by the detonation of atomic bombs over Nagasaki and Hiroshima and the ensuing nuclear arms race between the United States and Russia, the alleged relaxation of evolutionary selection due to advances in medical care and social changes that allowed survival of people who were genetically predisposed to medical conditions who might ordinarily have had no or few offspring, and the birth of babies with congenital conditions due to fetal exposure to rubella and thalidomide. Geneticists expressed their concerns for the quality of the human gene pool and the health of babies in the context of these issues and recommended various measures to ensure the genetic health of the population, such as greater access to contraception, reducing population growth, limiting exposure to ionizing radiation, and genetic testing and counseling. All while trying to distance themselves from eugenics.
The profession sometimes self-critically recognized its homogeneity but did not make concerted efforts to change the historical demographic profile. It was only over the last 5-10 years or so that more people have entered the profession who are non-White, of non-European ancestry, openly queer, live with a disability, are neurodiverse, and are male, even if the profession is still skewed toward its historical demographic. The newer less exclusive demographic has led to guiding ethical principals that focus on diversity, equity, inclusion, and justice within the profession and for the patients that genetic counselors serve. These issues are not unique to genetic counseling and are bitterly playing out in many social, political, and professional arenas.
Despite the increasing professonal diversity, several studies, personal recollections, and commentaries by genetic counselors from different backgrounds attest to the friction felt by both the “Old Guard” and the more diverse younger genetic counselors as these policies are implemented (or not) into training and clinical practice. Implicit biases abound in gatekeepers, supervisors, leading figures, research focus, and conferences. And, yeah, that includes me; far be it from me to cast the first stone. My generation of genetic counselors is very understandably criticized for the class, ethnic, and other biases of its practice, training, and ethos. The criticism hurts but probably because its core of truth makes us uncomfortable.
But at some point in the future, a fresh new generation of counselors will level a critique at the current practice, profession, and ethos of genetic counselors. and its focus on diversity, equity, inclusion, and justice. It is impossible to know what they will continue to embrace or decide to reject, or they might wonder how we could support certain viewpoints and practices, or shame us for some things, or criticize the language that we use. They will likely have a whole new set of issues that they feel will need to be freed from past baggage. Or maybe they will think the current generation is the apotheosis of moral practice (though I doubt it). As the history of medical genetics and genetic counseling illustrates, the ethos, morals, and clinical practice are always a microcosm of the larger socio-cultural environment. We are all situated within our eras and our ethnic and socio-economic context.
Though if we can only learn one constant about the history of genetics. it is that eugenics never goes away and it is always bad, whateve form it takes. We have to call it out when we see it, wherever it is. Maybe even in our own practice.
So let us practice ethical humility and recognize that even (especially?) highly ethical people have ethical shortcomings, difficult to admit to and often not obvious to us in the present but glaringly obvious with historical hindsight. We are all trying to do the right thing, even if we can’t all agree on what the right thing is. And the right thing changes over time, and we sometimes can’t appreciate when we are not doing the right thing. We are always on a journey, searching for ethical clarity.
*- The historical narrative is broadly similar in the United States, Canada, England and Australia. The history of genetic counseling in the rest of the globe is less well-studied but may not necessarily align with the narrative described here. Nonetheless, I suspect that the central concept of the current generation of genetic counselors passing judgment on the past will be true globally, although the details will differ.
**- Four of the captive Inuqhuit died in New York from acquired illnesses within a few months. The youngest, Minik, a 7 year old boy, was eventually raised as an adopted child of the museum’s chief building superintendent and somehow wound up working as a lumberjack in a small town in New Hampshire, where he died in his late 20s during the influenza epidemic.
by Ambreen Khan, Kim Zayhowski, Robert Resta, and Laura Hercher
This piece is our team’s account of censorship and threats from members of the genetic counseling community. It is both testimony and a demand that our profession do better. We were twice scheduled to present a webinar on the threat of modern eugenics – only for both events to be canceled after anonymous complaints and undisclosed claims about threats and safety. When organizations shield reputation over transparency, they marginalize dissent and chill scholarship that is essential to our clinical and ethical responsibilities. Institutional silence is not neutrality.
What actually happened?
Our webinar’s purpose was simple and urgent: to connect the historical roots of eugenics to the present. Genetic counseling partly emerged as a response to twentieth‑century eugenic abuses rooted in Francis Galton’s nineteenth‑century theories. We aimed to show that these ideologies are not relics but active influences – visible in the United States president’s eugenics-coded rhetoric, in technocratic visions of positive eugenics, and in colonialism and imperialism across the globe. We planned to demonstrate how sloppy science, genetic determinism, dehumanization, and essentialist language flatten human complexity and create openings for misuse; to interrogate whether elements of contemporary genetic counseling echo eugenic logic; and to engage participants in concrete strategies for explicitly anti‑eugenic practice.
Timeline of cancellation #1:
January 31, 2025: The proposal was submitted for the National Society of Genetic Counselors (NSGC) Annual Conference for a presentation on modern eugenics.
March 28, 2025: NSGC asked that the proposal be recast as a “Community Conversation” – a recorded webinar with a facilitated live discussion intended to extend reach.
June 4, 2025: We returned the revised proposal to NSGC. The final speaker team was Robert Resta, Laura Hercher, Ambreen Khan, and Kim Zayhowski. The live discussion was scheduled for September 29, 2025.
Summer 2025: We had many meetings as a presenter team about the content of each of our presentations. We assembled volunteer moderators, developed the session as a dialogic educational space, and stayed in regular contact with NSGC liaisons, sharing the slide deck and session plan for review.
September 4, 2025: The final recordings were submitted to NSGC, which were then posted for NSGC membership. We were informed several hundred people signed up for the event.
September 16, 2025: NSGC removed Ambreen Khan’s segment (“Reconsidering Eugenics through a Global Lens”) from the posted materials pending “fact‑checking” after complaints about alleged inaccuracies.
September 22, 2025: Following NSGC’s “fact-check,” the segment was restored with an appended reference list, and an overall disclaimer NSGC required stating that views expressed were the presenters’ own.
September 25, 2025: Four days before the scheduled live conversation, NSGC canceled the webinar and removed the recording. NSGC emailed the presenters and attendees, and referenced threats of violence to leadership and the organization as the cause of the cancellation. They provided presenters with no details, documentation, or evidence of those threats. Both emails said that the topic of eugenics would be addressed at a later date. NSGC paid presenters their honoraria.
October 6, 2025: One presenter followed up via email to request specific information regarding the nature of the threats, whether their source had been identified, what content provoked them, and if law enforcement had been involved. The presenter emphasized that, as a speaker for the upcoming annual conference, understanding any security risks related to the presentation’s content was essential for safely preparing future talks.
October 8, 2025: NSGC acknowledged that the questions were “very reasonable” and stated that the source of the threat had been identified and “addressed” with legal counsel, leaving “no ongoing concern.” They offered no specifics on the threats’ content, their origin, how they were handled, or what material had provoked them. Without these details, the presenter team could not evaluate their own safety for future engagements. To date, the talk has not been rescheduled and no explanation has been provided for why restoring the recording is not possible if the threat has been fully resolved.
Timeline of cancellation #2:
December 16, 2025: A genetic counseling graduate program’s Diversity, Equity, Inclusion, and Justice Committee reached out to the presenter team and invited a similar presentation on modern eugenics for a webinar open to genetic counselors and students. The event was organized by students and approved by program leadership for February 9, 2026.
January 28, 2026: The program emailed the presenter team and canceled the webinar, citing concerns about “belonging for all” and “potential lack of balanced perspectives” that they claimed would violate the university’s nondiscrimination policy, along with anticipated safety concerns. The email stated that the messages sent to the University expressing concerns had assumed the event’s material was the same as the Community Conversation referenced above. The program confirmed the content had not been fully reviewed before making the determination to cancel. One presenter noted that the cited university policy explicitly protects academic free speech even when it may provoke opposition or external pressure directed at the faculty or the institution. Promotional social posts (which had attracted 100+ likes and supportive comments) were deleted without announcing the cancellation.
Targeting and double standards
During NSGC’s “fact-checking” process, one speaker, Ambreen, was singled out for the portion of her presentation which analyzed genocides in the United States, Germany, Rwanda, and Gaza through the lens of medical ethics and eugenics. Complaints about her presentation were framed as questions of academic veracity. NSGC restored her content after review with appended references. In our view, this outcome indicates that the complaints were motivated less by demonstrable concerns about factual integrity and more by ideological opposition to her inclusion of Gaza and her critique of Israeli policies.
Ambreen and the Council on American–Islamic Relations (CAIR) sent NSGC a formal letter on November 10, 2025, urging procedural reforms. CAIR offered to help NSGC “review internal procedures for handling complaints to ensure that concerns about content do not serve as a pretext for suppressing marginalized voices or politically sensitive topics.” To date, more than three months later, neither Ambreen nor CAIR has received any acknowledgement or follow-up.
The CAIR letter underscored the harm of institutional repression, stating:
“One of the so-called citation concerns involved Ms. Khan failing to include a reference to Israel’s offer to treat Gazans in Israeli hospitals. It appears that Ms. Khan’s detractors simply disagree with her assertion that what Israel has done in Gaza is tantamount to genocide, which is a position they are able to hold and argue, but it should not result in the systematic silencing, censorship, and reputational harm to Ms. Khan. To be clear, Ms. Khan’s citations appear to be adequate; the disagreement appears to rest not on the veracity of her sources but on interpretation and analysis, which is within the scholarly discretion of any presenter. Singling out her presentation for heightened scrutiny and censorship has created a hostile and chilling environment for scientific and ethical dialogue. … Unfortunately, this is not the first time NSGC has censored members regarding the genocide in Gaza. We view this as an opportunity to engage in reasonable and appropriate restorative steps.”
What is at stake?
Censorship is not new to genetic counseling: our profession has navigated pressure over which histories, patient stories, and ethical critiques are acceptable to teach and debate. In recent years that pressure has intensified, playing out both publicly – high‑profile cancellations, wide-spread written petitions, and calls for professional sanctions – and privately, as quieter demands to remove material from syllabi, discourage certain research topics, or advise speakers to avoid specific language.
When educators and researchers preemptively “tone down” lectures, avoid case studies, or divert research away from challenging topics out of fear, they inflict a lasting corrosion of knowledge. Self‑censorship is the stealth weapon: curricula thin, research agendas narrow, and trainees learn that caution equals professionalism. Unlike an explicit ban, self‑censorship is invisible – until whole domains of knowledge vanish from professional discourse. That quiet retreat institutionalizes ignorance.
When a government or institution decides which ideas are acceptable, it ceases to be a sanctuary for inquiry and becomes a tool for social control. Across the world we see a coordinated strategy to suppress scholarship: in Hungary, the government outlawed gender studies to replace independent scholarship with state-sanctioned curricula; in India, the state uses police, laws, and bureaucracy to silence critics; in the United States, topics like Palestinian rights and Critical Race Theory are suppressed through legislation and institutional pressure.
This is not about ideological grandstanding; it is about clinical competence. Clinicians who cannot name the political and historical dimensions of eugenics are ill-equipped to safeguard patients from coercive programs or discriminatory allocation of care. Patients most at risk – disabled people, people seeking reproductive care, BIPOC communities, immigrants – pay the price. If our institutions silence education on the role of eugenic impulses in shaping border policy, how can genetic counselors recognize its modern iterations targeting immigrant patients? And if we cannot name Gaza or Sudan as sites where medical ethics are violated, what framework do we have to recognize – much less resist – the same violations anywhere else?
Teaching should be emancipatory, not neutral. Thinkers from Paulo Freire to bell hooks and Henry Giroux frame teaching as naming injustice and treating the classroom as a site of ethical resistance. The Palestinian ideal of Sumud (صمود) – a steadfast, rooted perseverance against erasure – extends this vision: learning itself becomes a daily act of standing against oppression.
Yet educational institutions too often prioritize procedural risk management over ethical clarity. When institutions invoke “safety” without sharing assessments or supporting speakers, the loudest and most aggressive opponents effectively decide what may be taught.
Eugenics thrives not only on coercive policy but on silence – on what is not taught, not researched, and not challenged. When institutions bow to intimidation and erase critical inquiry, they remove guardrails that might otherwise prevent discriminatory policies and coercive practices.
A call to action
We as a genetic counseling community must decide whether genetic counseling will be a profession that names power, confronts history, and defends the scholarship our patients depend on, or one that retreats into procedural silence when challenged. That choice belongs to all of us. The genetic counseling community does not have to, and should not, agree about everything but we should be able to respectfully, thoughtfully, and safely engage in debate and discussion.
Our team asks academic programs and professional societies to adopt the following policies to protect both safety and academic integrity:
Publish transparent moderation policies and threat-protocols
Make public criteria for removing or modifying recorded or live content, including what level of threat justifies cancellation and what evidence is required.
When “safety” is cited, share a summary of the threat assessment with presenters and with the membership (while protecting any legitimately confidential investigative details).
Include presenters in safety planning
Share threat assessments and possible mitigation strategies with speakers.
Collaborate on concrete steps (e.g., moderated Q&A, delayed posting, platform security, legal support) before deciding to cancel.
Provide visible, material support to targeted scholars
Offer logistical, legal, and public backing (e.g., an institutional statement affirming vetted content, assistance with security measures, and a designated liaison for harassment complaints).
Establish clear anti-retaliation policies for educators, students, and members who report censorship or advocate for reinstating removed content.
Create an independent appeals and review mechanism
Establish a review process for decisions to remove content or cancel events, with a timetable for review and public reporting of outcomes.
Commit to essential curricula
Ensure core training includes the political and historical forces shaping medical care in general and genetic counseling specifically, and defend those curricular commitments from suppression.
Remedy past harms
Publicly acknowledge cancellations that lacked transparency, reinstate or re-record content where appropriate, and issue formal apologies and restorative steps for presenters who suffered reputational harm.
Credible threats of violence are serious matters that deserve careful attention and response. Our demand is procedural: when safety is invoked, institutions must show evidence of due process, involve presenters in mitigation, and exhaust alternatives to cancellation before erasing vetted educational content.
In an era when threats are weaponized to control knowledge, yielding to intimidation forfeits our capacity to confront hard truths about power, policy, and medicine. Our duty is twofold: protect people from immediate danger and protect the integrity of knowledge itself. Silence may be easier, but it is a dangerous abdication. We are all responsible for the profession we build. Defend evidence. Defend teaching. Defend the people – patients, students, clinicians, and scholars – who depend on both.
Author note: This account is based on our direct involvement as presenters and on preserved documentation and correspondence with the institutions referenced. It reflects factual information available to us through our participation and our professional judgment. We remain available to address and correct any substantiated factual inaccuracies. The opinions and interpretations herein are exclusively our own and do not necessarily reflect the positions of our employers or affiliated institutions.
Jon Weil was Director of the Program in Genetic Counseling, University of California Berkeley, from 1989 to 2001 and is the author of Psychosocial Genetic Counseling, Oxford University Press, 2000. He retired in 2001 but has remained professionally active. His current interests include the continuing development of psychosocial genetic counseling and promoting locally focused, patient-oriented international genetic counseling.
Countertransference, defined broadly with respect to genetic counseling, “refers to conscious and unconscious emotions, fantasies, behaviors, perceptions and psychological defenses that the genetic counselor experiences as a response to any aspect of the genetic counseling situation” (Weil, 2010). Countertransference is important because genetic counselors confront the hopes, fears, anxieties and behaviors of patients in many forms, both major and minor. It can be a source of understanding, empathy and improved clinical practice. It can also be a source of personal pain and discomfort, including anxiety about one’s clinical efficacy. The topic of countertransference is addressed in many publications, from several perspectives (e.g., Biesecker et al., 2019; McCarthy Veach & Redlinger-Gross, 2025). Nevertheless, a new perspective is potentially useful, as the following vignette demonstrates:
As I ended a presentation on Countertransference in 2011, a student approached me with a question – “Could you think of countertransference as prior probabilities?” My response was immediate – “That is one of the most interesting questions I have ever been asked”. With time, my understanding of the value and perceptiveness of his question has grown.
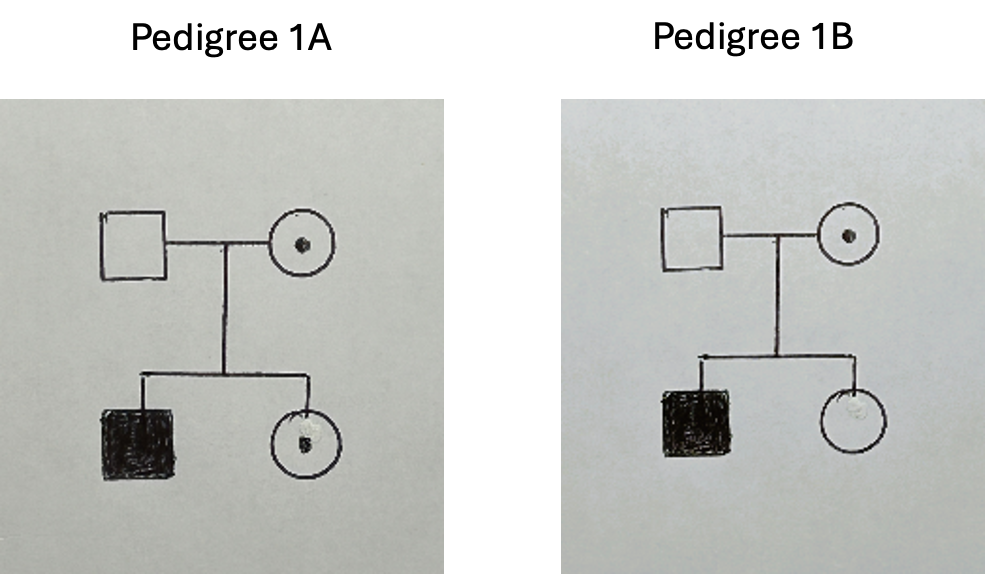
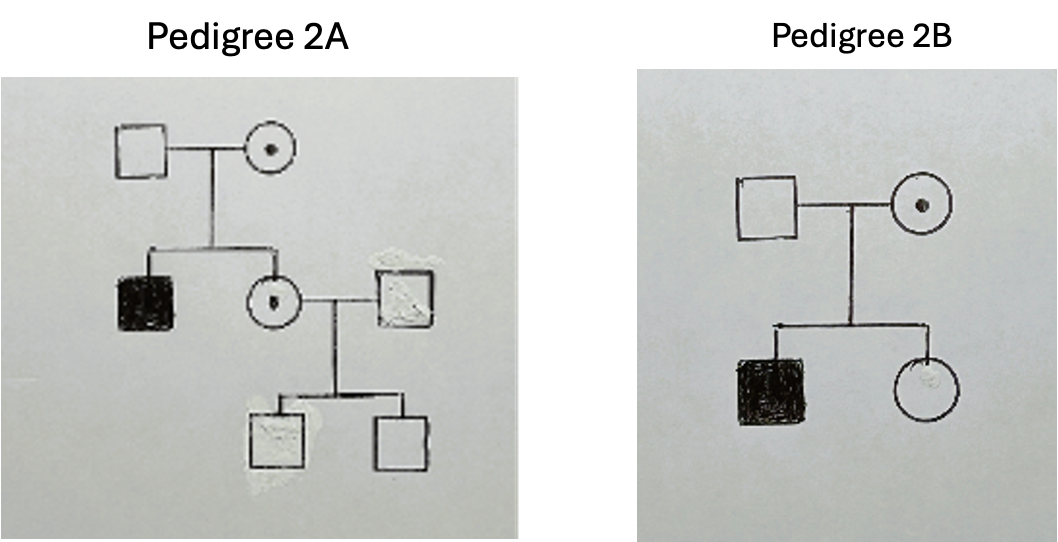
Bayesian analysis, to which the question referred, was critically important in clinical genetics and genetic counseling before DNA sequencing was developed (Hodge, 1998). Bayesian analysis uses “prior probabilities”, information that is subsidiary or “antecedent” to that presented in the counseling session, to adjust the calculated probabilities of the proband and/or other family members having a given genotype. For example, as shown in the following, the 50% probability that a woman whose brother has an X-linked disorder is heterozygous for the genetic variant (Pedigrees 1A and 1B; Table 1) is reduced to 20% by the additional, antecedent information that she has two unaffected male children (Pedigrees 2A and 2B; Table 2).
Table 1
Hypothesis
1A carrier
1B non-carrier
Probability
½ = 50%
½ = 50%
Table 2
Hypothesis
2A carrier
2B non-carrier
Prior Probability
½ = 0.5
½ = 0.5
Conditional Probability
¼ = 0.25
1 = 1.0
Joint Probability
1/8 = 0.125
½ = 0.5
Posterior Probability
.125/(.125 + .5) = 20%
.5/(.125 + .5) = 80%
A patient’s circumstances may also involve other forms of antecedent information. For example, for late onset disorders such as Huntington disease, the longer a family member lives without the onset of symptoms, the lower the probability that he or she carries the dominant genetic variant.
The parallels between prior probabilities and countertransference are intriguing. In psychological theory, countertransference involves experiences prior to the genetic counseling encounter that influence the genetic counselor’s cognitive and emotional assessment of the likelihood of potential interactions with the counselee (Weil, 2010). For example, a genetic counselor’s childhood experience with an angry parent increases awareness of a counselee’s growing anger during the course of a genetic counseling session. This in turn enables empathetic responses that reduce the likelihood of an angry outburst and promote a conversation that addresses the underlying issues.
However, it is when we look beyond these straightforward similarities that the broader heuristic value of the comparison becomes apparent. I believe there has been significant progress in promoting the value of countertransference in genetic counseling (Biesecker et al., 2019; McCarthy Veach & Redlinger-Gross, 2025). However, I assume that it still bears, to greater or lesser extent and in various settings, the onus of being a burdensome topic that, if not understood adequately, can lead to serious clinical errors and feelings of guilt and shame. Thinking of countertransference as antecedent information that adjusts the genetic counselor’s assessment of the probability of a patient’s possible thoughts or behaviors, thus improving the effectiveness of her or his interventions, provides another route to overcoming this onus.
Addressing countertransference can be difficult and distressing, bringing to consciousness painful experiences and emotions. These are best addressed with the assistance of an experienced supervisor or colleague or a licensed counselor or therapist. However, the analogy with prior probabilities allows some problematic aspects of countertransference to be reframed as issues of accuracy, reliability and representativeness:
There are a number of ways in which Bayesian analysis may produce erroneous results:
First, the data on which it is based may be incorrect and require subsequent revision (e.g., the diagnosis assigned to a forebear is incorrect, family understanding of the diagnosis is incorrect, and/or medical records are unavailable because they have been lost, are inaccessible in another country, etc.). Similarly, countertransference based on initial impressions or a specific attribute of the patient may prove incorrect or unreliable and require revision.
Second, the data may be used inappropriately. For example, for late onset disorders, age of onset data may be limited or not representative of the at-risk individual’s ethnicity. In the original formulation of transference and thus countertransference, it involved childhood behaviors and perceptions that offered the best solution to a difficult situation given the child’s position of powerlessness, but were less than optimal and could be significantly dysfunctional given that the adult’s situation is very different (Weil, 2010). Thus, we may compare countertransference grounded in perceptions and behaviors that are no longer relevant with Bayesian calculations based on data that are not representative of the situation to which they are applied.
Third, with complex pedigrees and/or multiple types of data (e.g., affected relatives and unaffected relatives with age of onset considerations), the calculation may be complex and one or more errors may have been made. Similarly, the complexity of a patient’s or family’s circumstances may induce countertransference that is not about the patient or family, but about the genetic counselor’s feelings of incompetence or of being overwhelmed, leading to responses that are not attuned to the circumstances.
The role of Bayesian analysis has receded and the understanding of countertransference has advanced since I was asked, a decade and a half ago, “Could you think of countertransference as prior probabilities?” However, thinking about countertransference in terms of accuracy, reliability and representativeness – as prior probabilities – may help reduce the anxiety and concern about making clinical errors that discussions about it, including in supervision, can evoke. It may help reduce the stigma that still attaches to countertransference, providing additional support for accepting it as a natural, inevitable process that is a potential source of valuable insight concerning the patient and the genetic counselor.
REFERENCES Biesecker, B. B., Peters, K. F. and Resta, R. (2019), Advanced Genetic Counseling: Theory and Practice, New York: Oxford University Press.
Hodge, S. E. (1998). A simple, unified approach to Bayesian risk calculations. Journal of Genetic Counseling, 7, 235-261
McCarthy Veach, P. and Redlinger-Gross, K. (2025) Genetic Counselors’ Personal Reactions and the Ethical Implications for Genetic Counseling Practice. In R. E. Grubs, E. G. Farrow and M. J. Deem (Eds.), The Oxford Handbook of Genetic Counseling. New York: Oxford University Press, pp. 516-530
Weil, J. (2010) Countertransference: Making the Unconscious Conscious. In B. S. LeRoy, P. McCarthy Veach and D. M. Bartels (Eds.), Genetic Counseling Practice: Advanced Concepts and Skills. Hoboken: Wiley-Blackwell, pp. 175-197
Autonomy has been a core guiding ethical principle of genetic counselors pretty much since the profession’s founding in the early 1970s. There are various definitions of autonomy but on a work-a-day basis in genetic counseling, it is usually conceptualized as the right of patients to make decisions about genetic testing that are educated and without undue external influence or pressure. It relies heavily on information-based consent. It is often, though not exclusively, evoked in the context of reproductive decision making, such as choosing whether to have children, whether to undergo prenatal testing and which test to have, and whether to continue a pregnancy if a fetal condition is diagnosed.
Reproductive autonomy in the context of genetic counseling was seen as an antithetical counterpoint to the Anglo-American-Germanic eugenic ideology of the first half of the 20th century and consistent with the wider trend in medical care to be patient-centered. But in a table-turning move, reproductive autonomy is now being used as an ethical justification for offering what many have called a modern version of eugenics – preimplantation polygenic screening of embryos for traits such as IQ, height, and eye color. I am not going to name the companies offering the testing because they don’t deserve or need the advertising. But the basic argument they make is that parents have an autonomous right to have children with the kind of traits that parents desire. Some people choose reproductive partners on this basis, so how is that any different than using a polygenic score?
The space between a trait and a mild medical condition, and between a mild versus a serious medical condition, is full of shades of gray but some of the traits that polygenic embryo testing screens for are clearly not medically signfiicant. Autonomy, as currently conceptualized, is unclear about which tests for which traits or medical conditions should be available to prospective parents or what ethical principles should guide parental choices.
Let me make my biases clear. I have a lot of criticism of preimplantation polygenic embryo screening. I don’t think that patients, children, or society benefit from the ability to select for these traits. The predictive value of polygenic screening for the traits is limited and questionable. And even if testing were reliable, is it worth tens of thousands of dollars to have a blue-eyed kid who is an inch taller and has an IQ 7 points “higher”? It almost sounds like a scam because parents will never know if their bundle of eugenic joy truly is taller or “smarter” than if they had just rolled the gametic dice.
I am also not convinced it will ever catch on to any large degree. Sure the ultra-wealthy can well afford it but IVF is a physical and emotional bear to go through (Note to those who push IVF on their partners) and a live birth often requires multiple cycles of embryo transfers. To say nothing of the higher incidence of pregnancy and neonatal complications associated with IVF, which is not entirely explained by parental characteristics. I also don’t like how preimplantation polygenic embryo screening has been subtly legitimized by giving it a set of initials: PGT-E (for preimplantation polygenic testing of embryos, just like PGT-A (for preimplantation aneuploidy screening), PGT-M (for monogenic conditions). Identifying something by its initials suggests that it is a common and widely accepted practice, which preimplantation polygenic embryos screening definitely is not.
Really, the threat to society is not preimplantation polygenic testing. The more serious threat is that a bunch of garden variety jerks with unimaginable wealth and power will raise a new generation of even wealthier and more powerful jerks who think they are privileged and God’s gifts to humanity. Someone should develop a polygenic score for being a jerk.
But back to the autonomy issue. Until now, challenges to autonomy stemming from which conditions should be available for prenatal testing have been raised before. Is it ethically acceptable for deaf couples to select for having a deaf child? What about a couple with achondroplasia choosing to terminate a pregnancy in which the fetus was of normal stature? These scenarios, not particularly common in clinical practice, were often evaluated from an ableist bias. Back in the 1980s, when amniocentesis and CVS were the only means of reliably determining fetal chromosomal sex, there was a general taboo against prenatal testing strictly for this purpose. This was a partially racialized ethic; not uncommonly, in the US the taboo was invoked in the context of Chinese or Indian parents but not typically for non-Asian parents who were nominally undergoing prenatal testing for “parental anxiety.” Now that fetal chromosomal or anatomical sex can be determined early and reliably in pregnancy, the ethical discussions seem to have been pushed aside because, well, I guess that information is now considered “fun” or “practical.”
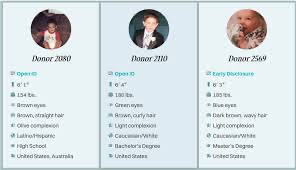
Preimplantation embryo polygenic screening to select for non-medical traits is, to some extent, a natural extension of the way that people have been choosing gamete donors for decades. Gamete donor profiles include a bewildering array of (usually unverified) donors’ non-medical traits such as demographics, educational attainment, reading preferences, and employment. This may in part be driven by patients’ emotional desire to choose a donor who might have the characteristics of person that the patient would have chosen to have a baby with if gamete donation was not necessary. But there is also an element of hoping that these traits might have a genetic basis and thus the child might share some of these same traits.
In the context of preimplantation polygenic embryo screening, the argument is made that patients are informed about the limitations of the predictive ability of polygenic testing and they are making knowledgable choices free of external direct pressure. For the moment putting aside the argument that commercial for-profit companies may not provide unbiased information and that there could be a certain amount of sales pressure, this is pretty much the same ethical justification used for any prenatal test. One ethical justification to rule them all. Although many of us may have the gut reaction that polygenic embryo screening is just plain wrong, there is little in this practice that violates the common conceptualization of autonomy.
In a challenge to the traditional conceptualization of autonomy, Ainsely Newson, Isabella Holmes, and their colleagues from the Universities of Sydney, Melbourne, and New South Wales recently offered up a different take on reproductive autonomy, a model that addresses some of the issues I raised above.* They delineate a conception of autonomy characterized by four attributes – qualtitiatve, relational, institutional conditions, and weakly substantive. These are outlined below, along with some thoughts on my part of how they might apply to preimplantation polygenic embryo screening.
Qualitative – the number of options offered to patients is less important than the quality of those options. Those options should be presented in ways that are consistent with patient values and such that patients are aware of the limitations of genomic testing in predicting what it means for their offspring. It requires good counseling skills to explore with patients what the traits in question mean for their lives and to what extent preimplantation polygenic screening of embryos reliably results in the promised outcomes. It also suggests that genetic counseling should not be performed by entities who have a financial stake in patients’ decisions. No criticism of the hard working, highly ethical genetic counselors, physicians, nurses, and other healthcare professionals who work for these companies, but, from a patient standpoint, a third party may be a preferable source of information.
Relational – No one exists in a social vacuum. Everyone is embedded in a social and economic context that can impact decision-making. Wealthy parents who are highly educated and have extensive resources may feel social and familial pressures to have children with traits that are presumably related to wealth and education. Conversely, less advantaged parents may feel pressure to offer their children as many biological advantages as possible, which they might think include higher IQ or being taller. Eye color? Well, that’s pretty much ethnically embedded. And everybody faces the pressure of having “a healthy baby,” a pressure intensified by advertisements that genetic testing helps assure a healthy baby.
Institutional Conditions – Patients need equal access to affordable health care, control over decisions about when and where to have children, and medical, educational, and financial resources. If everybody has equal access access to the same resources, then a test that predicts an inch of height or a few IQ points is less useful if the appropriate environment will have the same or even better effect.
Weak Substantivism – The process of how a patient makes a decision is less important than how it reflects the normative substance of the decision. In the context of preimplantation polygenic embryonic screening, the normative decision – “the right decision” – may be to have blue-eyed taller, higher IQ children, as imposed by the norms of a White Eurocentric majority. If instead a decision is made that is consistent with patient values rather than strong normative pressures, then it is weakly substantive.
The article is not an easy read for those of us less conversant with the bioethics literature; I had to read it a few times to get a handle on it. I freely admit I may have misconstrued some of their ideas and stand open to correction. But it is an excellent starting point for revisiting the concept of reproductive autonomy in the context of genetic counseling and how the concept of autonomy needs to be relevant to the current genomic universe.
Maybe too we should think about other ethical principals to consider in addition to autonomy. Complex decisions require complex ethics (I will leave that one for bioethicists and the Good Readers of The DNA Exchange to debate). We are living in the 21st century, not the 20th century. And God knows the world does not need eugenics.
_________________________________________________
The Holmes et al. paper use the term pregnant agent to refer to the pregnant person. This makes sense in the context of their ethical arguments about who has agency to make decisions about pregnancy and the complexities of who can carry a pregnancy and how pregnancy can be achieved.
I have been reflecting on the recent National Society of Genetic Counselors conference, and I hope to continue a conversation about one session in particular within our genetic counseling community. The session titled, “Hypochondroplasia Unmasked: Recognize, Understand, Advocate,” was an industry-sponsored session, which means that a company paid a fee to host the event. Attendees must reserve a spot for these sponsored talks, and they typically include a meal (in this case, breakfast). This talk, sponsored by BioMarin Pharmaceutical, was held on the first full day of the conference and was very well attended by a robust audience of genetic counselors and students.
BioMarin is best known for Voxzogo (vosoritide), which was granted FDA approval to increase linear growth for individuals with achondroplasia in 2021. Voxzogo is now approved for use from birth until the end of growth and is administered through daily injections at a cost of >$300K per patient, per year. The approval of this treatment, as well as the manner in which it has been tested and promoted has been controversial in the achondroplasia community. Little People of America, the world’s largest and oldest advocacy organization for people with dwarfism, has raised concerns over the FDA approval and focus on growth velocity, stating that this aim does not meet the health or quality of life needs identified by individuals with achondroplasia and that challenges related to height are mainly a result of social bias, discrimination, and lack of universal design. Those advocating for use of vosoritide speculate that increasing growth velocity may ameliorate some health concerns common to achondroplasia including sleep apnea and spinal stenosis; however, the actual effect is unknown at this time.
Hypochondroplasia is a skeletal dysplasia characterized by disproportionate short stature and mild joint laxity. Its presentation is highly variable, and individuals may reach an adult height that overlaps with typical stature. For this reason, hypochondroplasia may go undiagnosed. Of those who do receive a diagnosis, most people with hypochodroplasia have an identifiable variant in the FGFR3 gene. Variants in FGFR3 are also associated with achondroplasia.
BioMarin does not have an FDA-approved treatment for hypochondroplasia; however, they currently have an active phase 3 study to assess vosoritide in individuals with hypochondroplasia to determine its impact on growth velocity. The speakers at the NSGC sponsored-session seemed careful not to speculate about vosoritide treatment for hypochondroplasia; yet, the company is regularly talking about vosoritide use in hypochondroplasia with their investors. On a recent investor call, BioMarin projected the potential commercial launch date of Voxogo for hypochondroplasia in 2027. Chief Commercial Officer, Cristen Hubbard, shared a bit about BioMarin’s marketing strategy: “We’ve built the infrastructure, the relationships, and the expertise to execute effectively as new indications come online, and Voxzogo for the treatment of hypochondroplasia represents a potential significant breakthrough for patients. … many children go undiagnosed for too long, and that is why one of our priorities is improving early diagnosis for hypochondroplasia worldwide. We’re driving initiatives like genetic reclassification, clinician education, and patient and caregiver awareness, all aimed at driving earlier diagnosis. We’re also optimizing diagnostic pathways so that in the future, children can potentially access therapy as early as possible.”
As an attendee at the BioMarin sponsored talk, I have been thinking about how genetic counselors fit into BioMarin’s broader strategy. I believe the talk was intended to help build the relationships with genetic counselors given we often have trusted relationships with patients, families, other providers and health systems. They may also recognize that we support access to genetic testing. And I suspect they recognize that because we are often the first point of contact when a genetic diagnosis is made, we have significant influence over the initial information patients and families receive regarding resources and potential treatments.
In many ways, BioMarin is laying the groundwork for genetic counselors to facilitate earlier and expanded diagnosis of hypochondroplasia, while shaping a favorable view of treatment. This positioning seems aimed at ensuring a greater potential patient population in the event of FDA approval of Voxzogo for use in hypochondroplasia.
Of particular concern, the presentation appeared to frame hypochondroplasia in the most negative terms. Its intention likely being to frame the condition as serious enough to justify early diagnosis and eventual treatment for our patients, but BioMarin’s rhetorical choices troubled me.This presentation aimed to exploit the biases of the audience by emphasizing how shorter stature results in health, social, and emotional harms for people with hypochondroplasia and their families and was done explicitly with a narrative of burden.
In the opening outline, the speakers highlighted the first two key objectives of the talk were to “recognize hypochondroplasia and barriers to diagnosis”, and to “understand the burden and impact of hypochondroplasia.” An online poll at the beginning of the talk asked attendees to rate on a 10 point scale “how well do you understand the burden of hypochondroplasia?” Over 80% of respondents indicated that they did not understand the burden well with a response from 1-3 with 1 indicating “not at all”. One slide heading read, “Hypochondroplasia is a rare skeletal dysplasia that can impose a substantial burden on affected individuals and their families”. The speakers repeatedly emphasized the social stigma associated with shorter stature as a cause of psychological distress. This is particularly problematic given that social stigma is a product of societal discrimination and not a product of short stature itself. Attributing the burden of social stigma to a person’s body rather than societal discrimination reinforces ableist tropes that disabled bodies require fixing rather than calling attention to societal marginalization.
The presenters reviewed studies on quality of life scores which they used as evidence to justify that hypochondroplasia created a social and emotional burdens for families including difficulty in participating in daily activities, stress and feelings of social exclusion, and environmental barriers to development of autonomy. More progressive views of disability social justice would attribute these same findings differently and note evidence of accessibility barriers, lack of appropriate accommodations, and lack of community support, rather than problems inherent with short stature. This emphasis on the burden felt intentional, to exploit ableist assumptions about stature and disability to convince genetic counselors that competency in discussing hypochondroplasia involves framing short stature as a burden. Consequently, parents could be more easily persuaded that treatment of short stature through pharmaceutical intervention is then necessary.
At the end of the presentation the speakers repeated the same poll questions – “Following this symposium, how well do you understand the burden of hypochondroplasia?” This time the responses were almost reversed – nearly all respondents answered 8-10 on the 10 point scale (10 =“extremely well”). The presentation ended abruptly and the microphone was cut before anyone could ask a question. Indeed, when one of my colleagues did stand up to ask a question about the disability social-justice framing of the messaging, and the microphone was not turned on. We followed up with the speakers about the concern and were informed that they do not create the slides themselves but rather rely on BioMarin for the content and framing.
As genetic counselors we value helping families reach a diagnosis and support informed decision making about genetic testing and care. It is crucial that we critically assess where our information is coming from and the factors motivate the delivery of this information. We need to be attuned to our own biases and recognize when they may be exploited.
I urge my colleagues to recognize how our biases shape how we think and talk about the genetic conditions, testing, and treatment. Please consider carefully the source of the information you receive and seek out information and perspectives from people with lived experiences. As commercial interests in genetic testing and treatment expand rapidly, the choices we make about what information we emphasize, whose voices we center, and how we frame genetic conditions has the power not just to influence individual families’ decisions, but also to shape the societal discourse on diversity and disability.
My concerns about carrier screening for Duchenne muscular dystrophy (DMD) were first piqued during a presentation I attended at the Advances in Prenatal Molecular Diagnostics in November 2017. The presentation given by the chief diagnostic officer of genetic testing lab, Sema4, highlighted the lab’s experience with expanded carrier screening. Of 1,200 males in the series who underwent screening for both autosomal and X-linked conditions, Sema4 reported that five males in their 30’s-40’s were identified to have DMD variants interpreted as pathogenic for Duchenne. Upon follow-up, one reported a history of cardiomyopathy and four denied any symptoms or concerns related to DMD.
To learn that there were cases of adult males with pathogenic/likely pathogenic variants in the DMD gene, with most having no known symptoms in their 30’s-40’s, was surprising and confusing to me. This confusion primarily stems from what we have been taught and what continues to remain in current resources surrounding DMD – that penetrance for the condition is complete for males. It is possible that these individuals could have had subclinical Becker muscular dystrophy (BMD), and perhaps if evaluated they would have had cardiomyopathy or other symptoms that hadn’t yet surfaced to medical attention. But still, five males out of 1,400 screened is far higher than what we would expect with an estimated prevalence of ~1 in 5,000 male births with BMD or DMD per the CDC.
Sema4 also presented their finding of a very high carrier rate in females who were screened, with 1 in 522 females reported as carriers. This is far higher than anything that had been previously reported and also gave me pause as it would imply that about 1 in 1,000 males would inherit the DMD variant and the expectation to be affected, which is also much greater than what has actually been reported (and this doesn’t even account for de novo mutations).
What could explain this disparity between the high carrier frequency numbers, compared to the past reports of incidence and prevalence of these conditions? Perhaps it could be explained by variable expressivity and under recognition of individuals with subclinical BMD. Or perhaps, contrary to what we have thought, not all DMD variants are 100% penetrant in males? Maybe there is another genetic phenomenon that mitigates the pathogenic variants in some people? Could labs be over-calling DMD variants wherein many variants that are called pathogenic or likely pathogenic are actually benign?
An important study (Ding et al., 2025) published in Genetics in Medicine this month provides an explanation for some of the higher than expected carrier calls for DMD. The study highlighted that intragenic duplications in the DMD gene can be tandem or interspersed. Importantly, interspersed duplications often aren’t pathogenic. This brings forward an existing weakness in carrier screening, in that most clinical screening assays aren’t able to distinguish between tandem and interspersed duplications. Adding to this limitation are the current guidelines on variant interpretation that recommend to err on the side of assuming intragenic duplications are in tandem unless proven otherwise, a practice that has been named the “tandem presumption.” While this presumption may make sense when interpreting a duplication in a patient with clinical signs of the condition, what does it mean when we are making this tandem presumption with general population carrier screening, when patients have no symptoms or family history of the condition? According to the study, by applying the presumption broadly, many duplications will be incorrectly classified as pathogenic. The authors caution, “if the tandem presumption is inaccurate in these patients, it could lead to overestimation of variant pathogenicity—potentially resulting in unnecessary invasive procedures and/or pregnancy termination.”
Given that DMD has been included on expanded carrier screening panels for about a decade now, and we know that more “carriers” have been reported than makes sense when compared to the clinical prevalence of DMD-associated conditions, it seems highly likely that many people have made reproductive decisions based on DMD carrier results that may have been inaccurately assumed to definitively cause a dystrophinopathy. Five minutes searching Reddit for people’s experience with DMD carrier screening will give you a sense of how many people are agonizing about these results and what to do about prenatal diagnostic testing, whether to continue a pregnancy, or grappling with decisions around assisted reproductive technologies including IVF with preimplantation genetic testing.
Over the years, I have seen multiple patients with positive DMD carrier screening results, provided by more than one lab, and have noticed the following:
Some deletions and duplications reported on carrier screens are absent from the medical literature of people who have DMD-associated conditions. There are also some deletions that are seen in individuals with DMD-associated conditions, but exist on a spectrum from asymptomatic to mild Becker or isolated cardiomyopathy.
Lab reports typically don’t give any indication that these results are uncertain or incomplete; nor do they imply a possibility of variable expression or reduced penetrance. Lab reports typically provide a description of DMD and BMD with a very definitive prediction such as, “Each of this individual’s sons has a 50% chance of being affected and each of her daughters has a 50% chance of being a carrier.”
My follow-up calls to the labs to speak with a genetic counselor have confirmed that their internal data to the lab shows a much higher carrier frequency than we would expect based on the incidence of DMD-associated conditions.
I find these conversations with patients about DMD carrier results challenging because it often feels like my questions about the results are at odds with the wording included on the official lab report.
When I have the benefit of talking to patients about carrier testing before they proceed with it, I always discuss the possibility of uncertain information, even though that feature of screening is not clearly promoted as inherent to the test. Unfortunately though, most often we only have the opportunity to meet with patients after the results have returned, and I imagine that many with positive DMD carrier results may never meet with a genetic counselor at all.
Ding and colleagues offer a recommended decision tree for patients who receive results with a DMD duplication in the absence of personal or family history of dystrophinopathy. In this they recommend additional testing (long-read sequencing) to determine the structural configuration if possible. And if this is not possible they recommend familial segregation analysis. I hope that this study will prompt labs providing carrier screening to strengthen their protocols by recommending or providing additional clinical studies to clarify if these duplications are interspersed or tandem. If labs cannot do this, we need to be realistic about the complexity and time required in coordinating follow-up studies for patients with these results.
What is our role and responsibility of genetic counselors when considering DMD carrier screening? I believe any genetic counselors and any prenatal care clinicians involved in ordering carrier testing for patients should have careful conversations with patients prior to testing about the possible uncertainty that may arise from carrier screening results for not only DMD but from other conditions included on these panels as well. And in follow-up of positive results there are other steps we can take to help clarify the possible meaning of carrier results – not just with DMD duplications, but with all positive results.
I encourage all genetic counselors to reach out to advocacy organizations and colleagues with strong expertise in this area. It is understandable that many prenatal counselors don’t have the knowledge or time to complete or interpret literature reviews on a particular variant. Consider reaching out to colleagues through our NSGC Discussion forums or other trusted resources that offer peer contact. For example, the genetic counselors who work for Parent Project Muscular Dystrophy (PPMD) welcome contact from peers who need support in variant review.
I was thankful to recently learn that the genetic counselors with PPMD are open to helping with variant review and follow-up studies for families. PPMD manages the Duchenne Registry which holds genotype and phenotype data on thousands of patients with DMD and BMD, including mild and asymptomatic phenotypes. PPMD also runs the Decode Duchenne sponsored testing program, which provides both diagnostic testing and carrier or asymptomatic familial variant testing. This program may be utilized for cascade testing of both male and female relatives following a positive carrier screen. PPMD’s Genetics team, consisting of individuals who are certified genetic counselors, can often provide valuable information from their direct experience with the dystrophinopathy community.
The average age at diagnosis for Duchenne is between 4-5 and is often preceded by years of emotional, physical, and financial strain as parents struggle to find answers for their child’s symptoms. Identifying DMD variants may provide an opportunity for family planning and early treatment that is usually missed. As we learn that some DMD results are less straightforward than originally thought, it’s important that carrier screening results are carefully interpreted so that families who elect carrier screening can receive the benefits of this screening without introducing unfounded worry, or irreversible and potentially costly decisions based on misunderstood results. For now, it is up to our community of genetic counselors to help patients navigate these testing options and results and it is prudent for us to take a cautious and careful approach that goes beyond reading what is printed on the lab report.
I gratefully acknowledge the Parent Project Muscular Dystrophy Registry Team for their thoughtful review of this work and the valuable feedback that strengthened this post. I especially thank Ann Martin MS CGC, Kayla Banks MS CGC, Lauren Bogue MS CGC, and Katherine Anderson ScM CGC who provided detailed review and who also express their openness to collaboration in interpreting and following up on carrier screening results for our broader genetic counseling community. Their clinical expertise combined with resources to allow for variant follow-up and testing in families will improve and inform our approach to DMD carrier screening and follow-up for all.
There are many reasons people undergo DNA analysis. Medical decision making and risk assessment. Prenatal screening and diagnosis. Ancestry testing. Wellness and lifestyle advice so someone can reap profits off of largely useless data. Parentage testing. Police investigations. The analysis might involve different tests, such as sequencing your entire genome (give or take a few million base pairs), targeted portions of it, single gene sequencing, single nucleotide polymorphisms, or karyotyping, to name a few. The results are usually treated as a static bit of information that is an accurate representation of your genetic make-up throughout your lifetime. The implicit message often is that you are the external manifestation of this single DNA test, like a DNA sequence was a map with an arrow pointing at it with the message “You are here.”
But really, no test can come close to capturing all of the DNA in your body. Any one test or set of tests , while they may be highly accurate in the right hands, only capture a DNA sequence in a particular tissue(s) at a particular moment in the lifespan and is useful only for a specific reason such as cancer treatment, assessing disease risk, or reproductive decision making. It’s a snapshot taken with a single narrow lens for a single purpose, not an ongoing video using a multidimensional wide-angle lens. The snapshot could look quite different depending on which tissue is sampled or if the snapshot is taken at a different moment in time.
Let’s start at The Beginning, or actually, just before The Beginning. As the result of meiotic scrambling, maternal and paternal chromosomes will be distributed among the gametes in a bewildering mix of maternal and paternal contributions. Like about 8 million possible different combinations of maternal and paternal chromosomes. Estimates vary because who analyzes each oocyte in the fetal ovaries, but a 20-week female fetus probably has somewhere between two to eight million oocytes. In other words, it is possible that each of those oocytes has a unique combination of maternal and paternal chromosomes. The number of aneuploid oocytes in utero is unknown, but during reproductive years around 10% of oocytes are aneuploid or have an unbalanced structural aberration, with the percentage increasing with maternal age. Trinucleotide expansion repeats responsible for Fragile X syndrome and Huntington disease can arise in oocytes during meiotic prometaphase 1.
In a young male’s typical ejaculate, with tens to hundreds of millions of sperm, there is a higher but still low probability that maybe a few of those sperm will have identical maternal and paternal chromosomal contributions. But about 10-15% of sperm cells have chromosomal abnormalities, with perhaps 90% of those being structural rather than numerical. On top of this, de novo pathogenic gene variants can arise in any gamete, with the probability increasing with a paternal age. And no one has any idea of the frequency of de novo variants in non-coding regions in spermatozoa or oocytes.
Perhaps the only time in human development that we have a single genome is immediately at conception, although that may apply only to nuclear DNA since the mitochondria of the fertilized egg could be heteroplasmic. But as the fertilized embryo undergoes mitosis, different genomes arise almost immediately. Chromosomal mosaicism is detected in a significant number of embryos; anywhere between 2 and 40%, depending on a number of factors. About 2% of CVS specimens, which are derived from the fetal aspect of the placenta, are chromosomal mosaics. Mosaic single gene variants can also arise in neuronal progenitor cells, primordial germ cells, and other tissues. Fetal cells and cell free DNA work their way into in maternal circulation during pregnancy and the cells can persist in maternal circulation for years, a form of microchimerism.
Beyond conception and the embryonic period, somatic gene mutations regulary arise in fetuses, children, and adults in many different tissues. Some mutations are repaired, some persist and are clinically insignificant, and others make significant contributions to human disease. Cancer, for all intents and purposes, arises from somatic mutations. Cancer cells themselves then often go on to develop a bewildering array of mutations as the cancer grows and metastasizes. Mutation profiles can vary within the same affected tissue or between affected tissues. Further DNA damage can be induced by chemotherapeutic agents. Then there’s chromothripsis, where the genetic wheels come off altogether.
Clonal hematopoiesis of indeterminate potential (CHIP) is the result of somatic mutations in hematopoietic tissue and occurs in about 10% of people age 70 or older. CHIP is associated with an increased risk of many diseases, such as hematologic cancers, coronary artery disease, heart failure, stroke, and pulmonary disease.
X chromosome inactivation and mosaicism are another source of intra-person genetic variability. One X chromosome will be largely inactivated in anyone who was born with more than one X chromosome. This could have significant clinical effects, such as manifesting symptoms of Duchenne muscular dystrophy or hemophilia, often depending upon which X chromosome is inactivated and in which tissue. Furthermore, people with more than one X chromosome tend to lose one of their X chromosomes in some of their cells, especially as they age, such that they are X chromosome mosaics, which might lead to cognitive impairment.
The DNA of immune cells constantly alter themselves through processes such as somatic recombination and somatic hypermutation. This variability allows the immune system to respond in highly specific ways to so many different types of infection and cancers, and to help the healing process.
On top of all of this, we co-inhabit our bodies with all sorts of bacteria, viruses, protozoa, archaea and God knows what else, the composition of which changes regularly. In fact, most of the cells, and therefore most of the DNA in our body, are microbial (it varies at any given moment in time, like after a bowel movement). Since these microbes are symbiotic living parts of our bodies, their DNA is also our DNA.
Mitochondria are likely the remains of a microorganism that was integrated into host cells in our deep eukaryotic past. Mitochondrial DNA can be heteroplasmic, that is, any given mitochondrion can acquire a wide range of mutations that do not occur in other mitochondria. Heteroplasmy can be a significant source of medical conditions, depending on the degree of heteroplasmy and its distribution.
Intra-person genetic variability is one of the many reasons it is foolish and inaccurate to say that our DNA defines us. Each of us has many constantly shifting DNA sequences throughout our bodies and each sequence can play out in our lives in different ways at different times. The interaction of these sequences with each other and with our cellular, bodily, and external environments is so exquisitely and frustratingly complex that it is beyond comprehension by human or, I will wager, artificial intelligence (how could AI analyze the entirety of a person’s DNA sequences if it is impossible to capture all of those sequences at once, on top of which those sequences change over time?). Human beings are infinitely more complex than the near infinite sum of each of our body’s many genomes. We should all sing the body electric.
The love of the body of man or woman balks account, the body itself balks account – Walt Whitman, “I Sing The Body Electric”

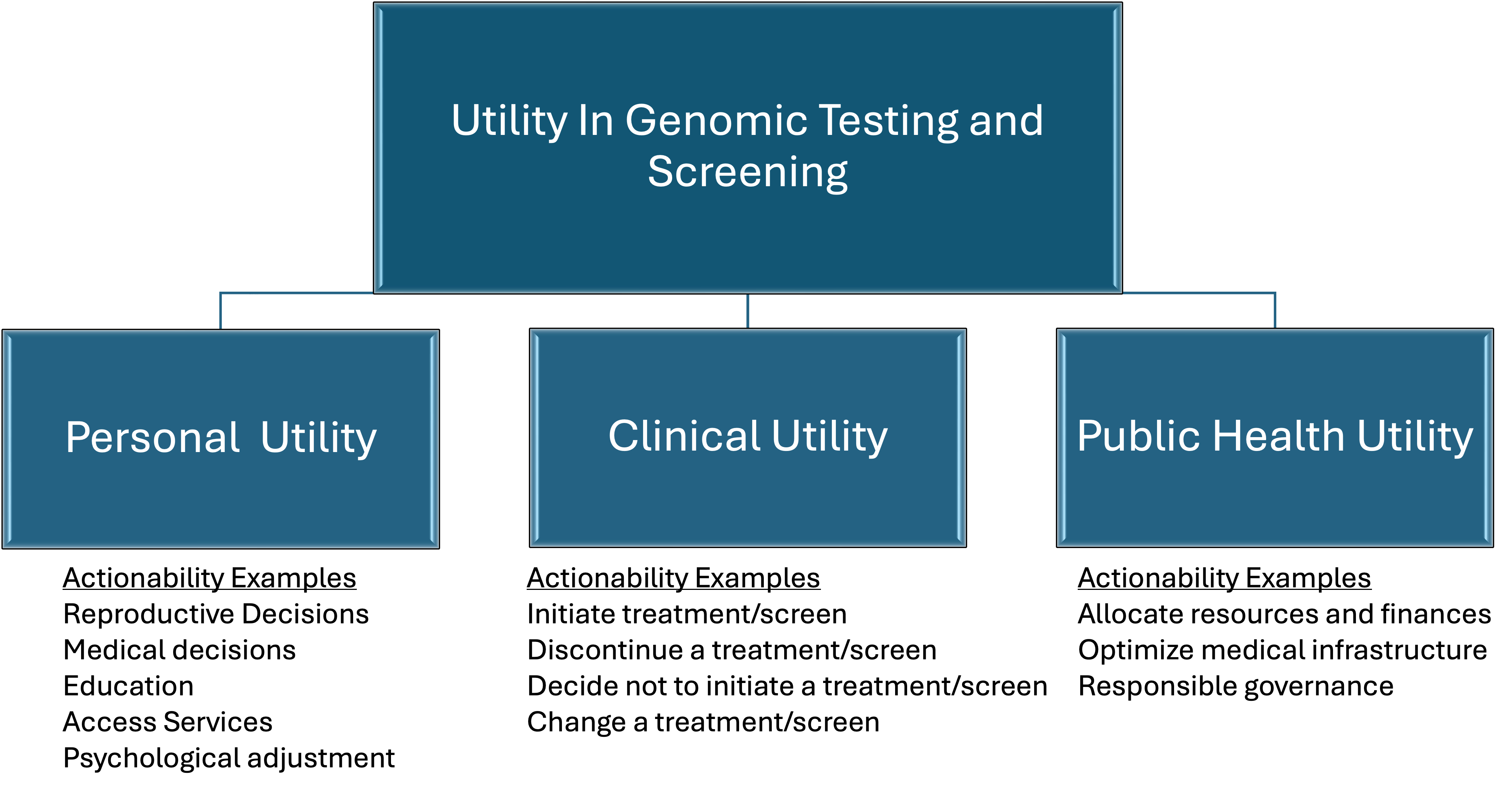
![The Barque of Dante (French: La Barque de Dante), also Dante and Virgil in Hell (Dante et Virgile aux enfers), is the first major painting by the French artist Eugène Delacroix, and is a work signalling the shift in the character of narrative painting, from Neo-Classicism towards Romanticism.[1] The painting loosely depicts events narrated in canto eight of Dante's Inferno; a leaden, smoky mist and the blazing City of Dis form the backdrop against which the poet Dante fearfully endures his crossing of the River Styx. As his barque ploughs through waters heaving with tormented souls, Dante is steadied by Virgil, the learned poet of Classical antiquity.
Pictorially, the arrangement of a group of central, upright figures, and the rational arrangement of subsidiary figures in studied poses, all in horizontal planes, complies with the tenets of the cool and reflective Neo-Classicism that had dominated French painting for nearly four decades. The Barque of Dante was completed for the opening of the Salon of 1822, and currently hangs in the Musée du Louvre, Paris](https://thednaexchange.com/wp-content/uploads/2026/04/image-13.png)