On Friday, November 22 Food and Drug Administration issued a warning letter to direct-to-consumer genetic testing company 23andMe. Many in the genetics community are experiencing a little déjà-vu this week, with the ensuing discussions in mainstream media and within online communities reminiscent of 2010 when FDA issued warning letters to 5 direct-to-consumer companies that were operating at that time. (Check out this post from Genomics Law Report for a good overview of the issue at that point in time.)
Regulation of direct-to-consumer genetic testing companies is complex and often confounded by thoughts and opinions regarding DTC advertising, DTC genetic testing, the validity and clinical utility of SNP-based panels, consumer rights and privacy, to name a few. I have personally fallen into a rabbit hole of articles, blog posts and twitter discussions in the past few days (see “Recommended Reading” section below). All of these outlets are debating the same issue, but this particular issue has an infinite number of very subtle angles.
The term “direct-to-consumer” conjures up strong emotions for genetic counselors. No doubt you will see some of this played out on The DNA Exchange in the next few days. However, in discussing the most recent FDA letter with a number of people (both colleagues and non-GCs) I’ve realized some basic review and clarification might be helpful. Hopefully this will serve as a nice starting point to frame our discussions on this issue in the days to come.
The full letter can be found on the FDA website here.
The 23andMe response has been posted here.
There are two basic aspects to the FDA letter:
1. Marketing
In the FDA’s words “…Your company’s website markets [your test] for providing “health reports on 254 diseases and conditions,” including categories such as “carrier status,” “health risks,” and “drug response,” and specifically as a “first step in prevention” that enables users to “take steps toward mitigating serious diseases” such as diabetes, coronary heart disease, and breast cancer….To date, 23andMe has failed to provide adequate information to support a determination that [your test] is substantially equivalent to a legally marketed predicate for any of the uses for which you are marketing it…”
My takeaway: 23andMe’s marketing materials claim their test can prevent serious diseases. The company does not have FDA clearance nor has it provided the appropriate evidence to make this blanket claim. This speaks most strongly to the clinical validity and utility of SNP-based testing—an issue that hits close to home for a lot of us. I think it is important that the FDA is highlighting the lack of evidence around prevention and predisposition testing for common disease. However, we need to recognize that 23andMe is also testing for additional variants beyond SNPs.
Anecdotally, I’ve noticed that genetic counselors continue to use the terms “direct-to-consumer genetic testing” and “SNP-based testing” interchangeably, which is both incorrect and adds to overall confusion. Genetic testing for common complex disease (primarily based on SNP information) is still controversial in our profession. However, as noted in the letter, 23andMe is a direct-to-consumer company that is also providing carrier testing for Mendelian diseases as well as the 3 common Ashkenazi Jewish BRCA mutations. To dismiss the 23andMe service by saying “this test doesn’t tell you anything!” undermines some of the routine testing that we do within a clinical setting. One cannot argue that 23andMe’s service “doesn’t tell you anything” and “has the potential for serious harm” in the same breath.
2. Direct-to-consumer health information
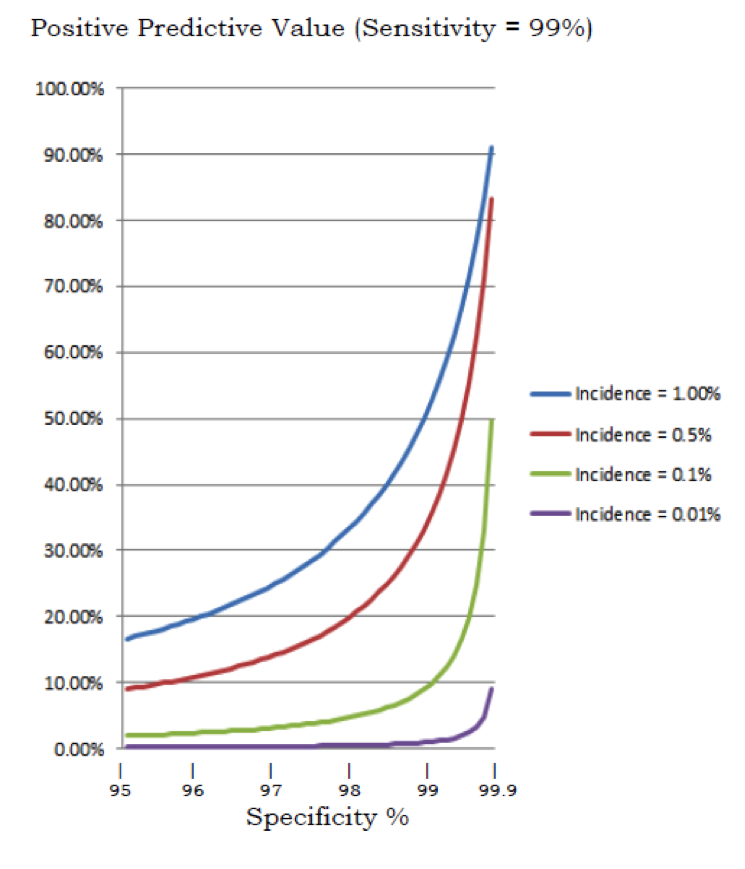
In the FDA’s words: “Some of the uses for which [personal genome service] is intended are particularly concerning… For instance, if the BRCA-related risk assessment for breast or ovarian cancer reports a false positive, it could lead a patient to undergo prophylactic surgery, chemoprevention, intensive screening, or other morbidity-inducing actions, while a false negative could result in a failure to recognize an actual risk that may exist.”
My takeaway: 23andMe is providing health information and test results directly to consumers without the involvement of a physician. This could lead to medical mismanagement, “serious injury or death.” I believe the DTC aspect of the testing (in comparison with the SNP-based aspect) is still the biggest challenge to the 23andMe model. Genetic testing for disease causing mutations without appropriate clinical context, family history review and individualized interpretation is where real potential for harm lies.
Suggested Reading (Or, some of the more interesting articles I have come across so far)
- Stopping 23andMe will only delay the revolution medicine needs
- It is game over for 23andMe, and rightly so
- FDA vs. 23andMe: How do we want genetic testing to be regulated?
Also, if you’re interested in learning more about FDA regulation of medical devices, I found this video on their website.









 for vagina
for vagina