Last week in Part 1 I looked at the potential impact of Trump’s policies on genetic counselors. Here I speculate about their impact on patients. As in my last posting, my analysis is not complete and, so far, mostly speculative because the effects of the policies are only beginning to be felt and Trump flip-flops so frequently that it’s hard to know how permanent they will be.
When that storm comes Don’t run for cover Don’t run from the comin’ storm
– Lyrics from “Storm Comin’ ” by Ruth Moody and released in 2011 by The Wailin’ Jennys*
I have often said that every genetic counselor and medical geneticist I have ever met would march into Hell for their patients and take on The Devil himself. Well, welcome to Hades. As bad as Trump’s policies are for genetic counselors and the larger medical, scientific, and research communities, patients are likely to fare far worse. Genetic counselors for the most part “only” have to worry about their jobs. Patients have to worry about their jobs, losing access to healthcare, reproductive healthcare, supplemental income, disease management, and life-saving treatment. As is the unfortunate par for the course, vulnerable populations will suffer the most – women, the poor, people living in rural areas, the elderly, documented and undocumented migrants, children, people with disabilities, LGBQT+ people, non-White people, and disabled veterans. The inhumanity of this is beyond comprehension.
Impact On Access To Health Insurance, Health Care, Social Service and Education
The claim that there are billions of dollars of Medicaid/Medicare fraud and waste committed by enrollees is blatantly false. The vast majority of fraud is committed by providers, not patients. And work-requirements for Medicaid recipients are laughable and only feed into the myth of a large body of “undeserving poor.” 65% of people on Medicaid work but typically in jobs with low salaries and no health benefits. Those who don’t work do so because they are disabled or ill, are attending school, or are caregivers. The work requirement implemented in Georgia a few years ago resulted in the majority of Medicaid money funneled toward covering administrative costs for the work requirement program rather than needed services for enrollees. If you are serious about saving significant amounts of money in the Medicaid program, go after the providers and the state administrators, not the recipients.
The Department of Education has lost nearly half its work force since Trump took office, with the most recent firings on March 11. Further funding and personnel cuts are likely in the near future, with possible elimination of the department altogether. The Department of Education’s Office of Special Education Programs funds grants to states that then distribute the funds to local school districts. In 2023, this amounted to $18.4 billion in aid. Many children with developmental disabilities rely on state-funded educational intervention programs to help them achieve their full potential.
Immigrants, documented and undocumented, may lose access to Medicaid due to funding cuts and anti-immigration bias. About 50% of undocumented immigrants and about 1 in 5 lawfully resident immigrants lack employer-sponsored health insurance even if they are employed. Not only do they face restrictions and barriers to accessing government-sponsored health insurance, they may not even want to seek health care out of fear of being deported. Oh, for those who say they don’t want their tax dollars going to insure immigrants, in 2023 undocumented immigrants paid about 90 billion dollars in local, state, and Federal taxes. And, if they are legally employed, they pay into Medicare but are not usually eligible to receive Medicare benefits.
Why the need to persecute people who are gay or transgender or whoever isn’t cis-heteronormative? Can’t you just let people try to lead their lives and loves in peace and good health, and leave them alone already? Life is hard enough as it is.
From a practical political standpoint, it’s difficult to understand how these moves will help Republicans win votes in future elections at the state and federal levels. Medicaid and Medicare covers over 100 million people of voting age, and another tens of millions of voting age adults are LGBQT+, for a total of well over 100 million voting age adults. In the 2024 election, 155 million people voted altogether. If these groups united behind a presidential candidate who promised not only to restore but expand those benefits, the candidate would win in a true landslide (unlike the landslide victory that Trump keeps claiming, which was actually one of the smaller victory margins since the 19th century). But people often do not vote in their own best interests or just don’t vote at all so it’s hard to know how this will play out in the ballot box.
Impact On Reproductive Healthcare
“I said, ‘Well, I’m going to do it, whether the women like it or not,’” Trump said. “I’m going to protect them.”
The situation is just as dire for access to reproductive health care. As noted above, Medicaid covers about 40% of births in the United States overall, increasing to about 50% of births in rural areas. Medicaid cuts will likely further the closure of hospitals in rural areas, where hospitals depend more on Medicaid funds than in large metropolitan areas. This means that there will be loss of obstetric services in poorer rural areas (and other medical and mental health services too), so women will have to travel further to deliver their babies. Loss of childbirth coverage will likely result in more health problems for mothers and babies, and further contribute to US neonatal and maternal death rates, which is among the highest in the world. The maternal mortality rate is particularly high among Blacks; about 65% of Black women are covered by Medicaid.
Trump takes credit for overturning Roe v. Wade, a ruling which has led to extensive abortion bans around the country. It seems likely that the extent and number of bans will increase over the next few years, backed by support from Mordor The White House. But the administration’s policies extend beyond abortion to birth control and research about maternal health outcomes. Executive Order 14182 signed on January 28 rescinded two of Biden’s Executive Orders, the consequences of which include:
•Dismantling the Interagency Task Force on Reproductive Healthcare Access, which had been established to ensure a whole-of-government response to the crisis
•Stopping federal agency efforts, specifically by the Department of Justice, the Department of Homeland Security, and Federal Trade Commission, to protect patient and provider privacy and security
•Halting agency efforts to enforce anti-discrimination law in response to reports of people being denied emergency abortion care and prescription medication
•Stopping federal agency efforts to ensure individuals receive emergency abortion care as guaranteed by law
•Ceasing efforts to advance abortion access for patients enrolled in Medicaid who must travel for abortion care
•Stopping public education and awareness efforts about access to reproductive health care, including informing people about how to obtain birth control;
•Blocking data collection, research, and analysis in measuring the effect of access to reproductive health care on maternal health outcomes and other health outcomes.
They may as well have put The Taliban in charge of women’s reproductive health care policy.
On its face, Trump’s Executive Order increasing access to IVF appears to be a win for reproductive healthcare since many private insurers provide minimal or no coverage for this service. However, the order only recommends that “Within 90 days of the date of this order, the Assistant to the President for Domestic Policy shall submit to the President a list of policy recommendations on protecting IVF access and aggressively reducing out-of-pocket and health plan costs for IVF treatment.” It lays out no concrete strategy for raising the funds to cover this expansion or forcing insurers to cover it, and makes no mention of coverage for other assisted reproductive technologies (ART). More critically, the Executive Order may wind up limiting access to IVF. Vince Haley, who is the Assistant to the President for Domestic Policy and responsible for creating the recommendations, is a former assistant to Newt Gingrich, a speechwriter for Trump under the supervision of Stephen Miller, who is virulently anti-LBGQT+ and anti-immigrant. Hence Haley’s policy recommendations will likely exclude LGBQT+ people and unmarried heterosexual people from having access to IVF. I wouldn’t be surprised if the policies also exclude immigrants, given Haley’s connection to Stephen Miller, the administration’s emphasis on pronatalist policies, and Trump’s allusions to “white replacement theory.”
Robert F. Kennedy, Jr., the head of the Department of Health and Human Services, has made a career of spreading lies, inaccurate claims, and misinformation about vaccines. His anti-vaccination stance could result in fewer women and chlldren getting the MMR vaccination or the varicella vaccination if they are infection-naive adults. This could in turn lead to an increase in the incidence of congenital rubella syndrome and congenital varicella syndrome. If a mother acquires measles during pregnancy, it could lead to serious consequences including death, pneumonia, miscarriages, stillbirth, prematurity, and low birth weight. And cod liver oil, Kennedy’s preferred treatment for measles, contains high levels of vitamin A, a potent human teratogen.
Impact On Income
Proposed cuts to Social Security could have dire consequences for people with disabilities and their families. Social Security Disability Insurance (SSDI) provides supplemental income to adults and children with disabilities. It is the only federal financial program for this group, and serves only the lowest income families whose children have conditions such as Down syndrome, cerebral palsy, autism, intellectual disability, and blindness. Families receive about $800 a month on average. The families are so poor that even shaving a few dollars off that amount could have profound effects. These cuts are being proposed by the world’s richest man who sells trucks that cost at least $100,000 each and gets free advertising at the White House. Yeah, he’s tuned in to the needs of low income families and people with disabilities.
Cartoon by RJ Matson, editorial cartoonist at Roll Call, a newspaper covering Congress and Capitol Hill. Source: The Contrarian https://contrarian.substack.com
Impact From Limitations And Cuts To Clinical and Genetic Counseling Research
Funding and personnel cuts at the NIH would be another blow to the care of genetic counselors’ patients. The NIH, and particularly the National Human Genome Research Institute (NHGRI), are key sources of clinical and other research programs focusing on hereditary disorders. In particular, it specializes in people with rare disorders and serve as a resource for the families and their healthcare providers who have nowhere else to turn to. NIH and NHGRI helped establish and maintain the Undiagnosed Diseases Program, which is instrumental in providing diagnoses and care recommendations for people who have been seeking a diagnosis in vain, sometimes for decades. Most of the stunning advances in the treatment and care recommendations for rare genetic diseases are based on research performed at this Institute.
Patients would also be negatively affected by the loss of NIH-funded genetic counseling research that examines the pychological, familial and medical impact of diagnosis, treatment, and management of genetic conditions on patients and their families. The value of cutting edge clinical research would be blunted in the absence of the best way to implement discoveries into the lives of patients so they can get maximal benefit. Any cuts to NHGRI would be keenly felt by patients with genetic conditions.
We cannot be lulled into a sense of powerlessness and inevitability about these policies. We can’t only rant and rave. We need some radical optimism. We need to fight back tooth and nail in small and big ways. We need to encourage our patients and colleagues, at least those who are not vulnerable and deeply threatened by the political climate, to let their government representatives know in no uncertain terms that these policies are unacceptable and that their political futures hinge on sane and compassionate policies. We need our professional organizations – NSGC, ACMG, ASHG – to start collecting data in an organized and coordinated fashion to document specific situations and cases where the policies have negatively affected patient care and the practice of medical genetics and genetic counseling and broadcast it far and wide. Let’s put Hell back where it belongs.
– For some reason, these days I am favoring Canadian musicians. Lots of time listening to the Wailin’ Jennys, Joni Mitchell, Leonard Cohen, Kate and Anna McGarrigle, Rufus Wainright (son of Kate McGarrigle), Neil Young, Alanis Morisette, Drake…. I could go on but I don’t want to sound too Tragically Hip. You can take Joni’s line from Big Yellow Taxi and apply it to democracy “Don’t it always seem to go that you don’t know what you’ve got ’til it’s gone?”
This is a two part blogpost. Part 1 focuses on the impact of Trump’s policies on genetic counselors. Part 2, which I plan to post next week, will focus on the impact on patients.
When everyone is up front and they’re not playing tricks When you don’t have no freeloaders out to get their kicks When it’s nobody’s business the way that you want to live Oh my mama told me There’ll be days like this (From “Days Like This” by Van Morrison, 1995; not to be confused with the delightful Shirelles 1961 song with a similar name)
Many genetic counselors are zombie-shocked over the cruel, thoughtless, and harmful policies of Donald Trump (Pronouns: I!/ME!/MINE!). Genetic counselors hold a broad range of political beliefs but most tend to lean left. But liberal and ultra-conservative genetic counselors share a common set of values around patient care, as embodied in our Code of Ethics, re-enforced during our training, and laid out in our textbooks. So even if you support some of Trump’s non-medical policies, surely there should be near universal condemnation, or at the very least concern, over the implications of Trump’s policies for our profession and our patients.
Much of what I discuss below is speculation on what may happen and is not meant to be an exhaustive analysis. The policies are for the most part new and are only starting to impact medical care. Some are working their way through the court system but it remains to be seen how the rulings will turn out and if the Administration will ignore them. Also, the policies tend to change with, as far as I can tell, the direction of the wind (see tariffs). Hopefully, my speculation and predictions will not fully pan out.
First off, the employment of many genetic counselors is at stake. Genetic counselors who work at the National Institutes of Health (NIH) or the Department of Veterans Affairs or other federal agencies such as the military may have their positions may be eliminated by the reckless DOGE budget cutting antics (putting Musk in charge is like hiring Moe, Larry, and Curly to make your car run more efficiently. Man, wouldn’t you like to take a wrench to his nose). In addition, the salaries of some genetic counselors
engaged in research are fully or partially funded by federal government grants. With the cancellation of research proposals that address DEI in any way shapeor form – even if DEI is only mentioned in the proposal – or allude to any of the many other topics that get Donald’s knickers in a twist, funding for these positions may be lost. The employment effects may be further worsened as Trump targets federal funding for universities that don’t conform to his distorted view of the world, such as the recent canceling of $400 million in federal funds allocated to Columbia University under the guise of concern for harassment of Jewish students on campus. The safety of students is a serious concern to be sure, but cutting off funding is just an attempt to stick it to a “woke” university. All this at a time when the job market for genetic counselors is less than ideal.
The underlying economics of genetic counseling services will likely hinge on genetic counselors becoming covered providers under Medicare. The National Society of Genetic Counselors (NSGC) has been working for over a decade to achieve this goal, which seems to be frustratingly closer but not quite there every year. As I noted in a previous post, should the Access to Genetic Counselor Services Act actually come up for a vote in Congress, congressional members may reject it because of NSGC’s DEI policies, as clearly articulated in its gender-first pedigree nomenclature Practice Resource. The profession may miss out on becoming Medicare-covered providers because we are trying to be decent human beings who respect the dignity of our patients.
Trump’s policies on limiting the funding NIH research has the potential to impact the types of research that genetic counselors can engage in or benefit from, especially if some aspect of DEI is involved. The net effect will be delivering sub-standard and unresearched care to some of our most vulnerable patients. Here are the NIH research funding guidelines, as outlined in a recent NIH memo:
Category 1 – The sole purpose of the project or conference is DEI-related – WILL NOT FUND Category 2 – Projects or conference that partially supports DEI activities – WILL FUND ONLY IF THE DEI ACTIVITIES ARE ANCILLLARY TO THE PURPOSE OF THE PROJECT AND ARE ELIMINATED FROM THE GRANT Category 3 – Project or conference that does not support DEI activities but may contain language related to DEI – WILL FUND ONLY IF DEI LANGUAGE IS REMOVED Category 4 – Project or conference that does not support any DEI activities – CAN BE FUNDED.
And here are the justifications for these guidelines, from an appendix to the same memo:
DEI: “Research programs based primarily on artificial and non-scientific categories, including amorphous equity objectives, are anti-thetical to scientific inquiry, do nothing to expand our knowledge of living systems, provide low returns on investment and ultimately do not enhance health, lengthen life, or reduce illness. Worse, so-called diversity, equity, and inclusion studies are often used to support unlawful discrimination on the basis of race and other protected characteristics, which harm the health of Americans.” Transgender issues: “Research programs based on gender identity are often unscientific, have little identifiable return on investment, and do nothing to enhance the health of many Americans. Many such studies ignore, rather than seriously examine, biological realities.”
How much does the Republican Party hate LBGQT+ people? During the 2024 campaign, it spent one quarter of a billion dollars on anti-transgender and anti-LBBQT+ advertising. This is a policy of pure hate and part of the attempt to legislate LGBQT+ people out of existence. Call it administrative genocide.
Trump’s policies also have direct bearing on how genetic counselors document patient encounters in the medical record. Being identified as transgender or non-cisgender or non-heterosexual places patients in a very vulnerable position. Once could easily imagine the government obtaining a warrant or whatever legal document to obtain the medical records of any of our patients; HIPAA guidelines allow healthcare providers to release records without patient permission “as required by law (including court orders, court-ordered warrants, subpoenas) and administrative requests.” An Executive Order signed on January 28, among other horrible things, proclaims that it “Stops federal agency efforts, specifically by the Department of Justice, the Department of Homeland Security, and Federal Trade Commission, to protect patient and provider privacy and security.” Now imagine if a patient had gender-affirming care in a state where it is banned. This puts genetic counselors in a very difficult position. On the one hand, knowing if a person is transgender or non-heterosexual can be important for their healthcare guidance and genetic counseling. On the other hand, documenting that information in the medical record can potentially bring great harm to patients. This is going to require some awfully complex and sensitive discussions with patients. But mostly it will probably just discourage them from seeking medical care. Think I am exaggerating? Well, recall that in 2023, Tennessee’s Attorney General forced Vanderbilt University Medical Center to hand over the medical records of their transgender patients.
This same dilemma holds true for documenting the medical, reproductive and family histories of patients who have undergone a termination of a pregnancy, particularly in states with strict anti-abortion laws. The patient or the provider who performed the abortion could face jail time.
Trumpian attempts to remove “unacceptable” DEI language from federal government discourse and to force federal agencies to modify the information they provide to conform with the president’s views and policies threatens the utility or even the very existence of some of the reference tools and research projects that genetic counselors rely on every day. If we can no longer believe a word that comes out of the mouth of the president or his representatives, and if his policies affect what can be said by government agencies, how are we to trust the content of PubMed, ClinVar, ClinGen, the Morbidity and Mortality Weekly Report and other CDC publications, etc.? What will become of the Metropolitan Atlanta Congenital Defects Program, which was established in 1967 by CDC to monitor the incidence of congenital conditions in the Atlanta area or the National Birth Defects Prevention Network, which maintains a national network of surveillance of congenital conditions? What will be the fate of the International Clearinghouse for Birth Defects Surveillance, a CDC-sponsored program which brings together birth defects monitoring programs from around the world? Maybe the DOGE apparatchiks, in all their glorious ignorance and hubris, will just eliminate them altogether.
Trump’s policies could threaten the safety of some genetic counselors in their workspaces. They may now feel physically and psychologically unsafe at work, particularly those who are not White or heteronormative. They don’t know if their employers will protect them or fire them. Co-workers may blame them for budget cuts that result from decreased federal funding or accuse them of being “DEI hires.” They may be concerned that patients will feel free to harass, criticize, abuse them, or even report them to “the authorities.”
Genetic counseling has a history embedded in eugenics, a history that the profession has tried to disentangle itself from. Here we are again, having to confront the specter of eugenics in our midst. In another chapter from the book titled “We Don’t Learn Any Lessons From History,” the policies and rhetoric of Trump et al. channel the spirit of the Eugenics Record Office. Republican labeling of immigrants as rapists, thieves, genetically inferior, and of low intelligence is the exact same language employed by early 20th century eugenicists to describe, among others, Italian and Eastern European immigrants “flooding” the country (incidentally, my grandfathers were born in Italy and Poland but managed to arrive before the 1924 Johson-Reed Act put extreme limits on the number of immigrants allowed from those countries). Ultra-conservative eugenicists, such as Madison Grant in his 1916 book The Passing of the Great Race, stoked fears of “White Replacement” whereby Northern and Western European American stock would be replaced by large numbers of undesirable immigrants and their many offspring (at the time, Southern and Eastern Europeans were considered a separate race from people of Anglo-Saxons and Scandinavians). So too do Trump, Musk and their ilk seek to limit immigration, deport immigrants, and push pronatalist policies that encourage “native-born Americans” to have more children.
“Leave now. If you don’t, we will find you and we will deport you. You will never return.” Kristi Noem, Secretary of Homeland Security, from a TV commercial threatening immigrants
“Give me your tired, your poor, Your huddled masses yearning to breathe free, The wretched refuse of your teeming shore. Send these, the homeless, tempest-tost to me, I lift my lamp beside the golden door!” – Emma Lazarus, The New Colossus
I have heard grumbling from some genetic counselors that they are upset by the lack of a strong voice and policy action from NSGC. They want to know just where their professional organization stands on these issues and how it will support its members and the patients they serve during these tumultuous times. NSGC claims to be committed to DEI issues, and this is a test of the organization’s sincerity and willingness to fight for their principles. The grumbling genetic counselors may have a point.
On the left is a political cartoon from 1903; on the right is a political cartoon from The Chattanooga Times from 2010.
Of course, all these policies and Executive Orders affect the care genetic counselors can provide to our patients, who will suffer the most. I will take up the topic of the impact on patients in the next week or so in Part 2.
This Friday, March 14th at 4 PM EST, several genetic counselors are independently organizing a mutual support zoom call for genetic counselors to share in a safe and supportive space their stress, anger, frustration, views, anxieties and whatever other emotions they are experiencing as a result of the Trump insanity. If you are interested in attending (no participation required), contact Jehannine (J9) Austin (jehannine.austin@ubc.edu) or Kate Wilson (kate.genetics@gmail.com) or if you are on BlueSky, Naomi Wagner (@naomi-cgc-bsky.social).
In a previous posting I suggested some actions and organizations that genetic counselors can consider doing or joining if they feel the need to fight back in some way. Jill Fonda Allen has since offered one other organization to consider getting involved with – Indivisible, which, per their website is “a grassroots movement of thousands of local Indivisible groups with a mission to elect progressive leaders, rebuild our democracy, and defeat the Trump agenda.”Thank you, Jill.
In this post, the word “fat” is used intentionally to follow the language of fat advocacy organizations. This is meant to challenge the notion that the word “fat” is inherently bad but rather is a neutral descriptor that describes the bodies of many people. As with other identities, individuals may prefer the use of other terms to describe themselves, in which case it is always best to mirror that language.
Genetics is at the core of many efforts to address the “obesity epidemic.” Genetic tools such as polygenic scores, CRISPR-Cas9 technology, and direct-to-consumer genetic tests share the goal of minimizing fatness. Not only do these efforts ignore the already understood social determinants related to weight and health, but they consistently exclude the perspectives of fat people. Additionally, gene panels designed to identify monogenic causes of obesity raise concerns; while they might be able to provide actionable medical information, the focus should not be exclusively on weight loss.
When we center weight loss as the main mechanism to support one’s health, we reinforce the persistent idea that if someone is fat, they are, by definition, unhealthy, and addressing their weight, therefore, must be a top priority. This can lead to experiences where people’s health concerns are not taken seriously or further explored, perpetuating mistrust in the healthcare system and subpar care. As the genetic counseling profession strives to promote more inclusive and equitable spaces, it is important for us all to reflect on our own biases and minimize over-pathologizing fatness.
Anti-fat bias is pervasive
Fatness is unique in that it is both externally visible and it remains socially acceptable to point out or express dislike for. One’s weight is often attributed to a direct depiction of a person’s character or behavior. Fat people are seen as “lazy” and “lacking willpower,” while thin people are perceived as having “earned” their societal advantage. In her book Hunger, Roxane Gay writes,
“When you’re overweight, your body becomes a matter of public record in many respects. Your body is constantly and prominently on display. People project assumed narratives onto your body and are not at all interested in the truth of your body, whatever that truth might be. Fat, much like skin color, is something you cannot hide, no matter how dark the clothing you wear, or how diligently you avoid horizontal stripes” (page 31).
Media reinforces these beliefs. Popular films and TV shows such as Super Size Me and The Biggest Loser present opportunities for viewers to pass judgment on those who engage in “fattening behaviors” while further solidifying one’s pre-existing belief that thinness is earned by a series of correct decisions. Even in the recently released Wonka, fatness stemming from gluttony, selfishness, and poor morals is used repeatedly as a punchline. News coverage of the so-called “obesity epidemic” is filled with unflattering images of “headless” individuals, often sedentary or eating “unhealthy” food. Imagery such as this works to remove the humanity of people who are fat and further the widespread belief that fatness is simply a result of “bad choices.”
Similar to other forms of oppression, people experience anti-fat bias in many ways. For example, there currently exists no federal protections and very few state protections against weight-related discrimination in the workplace. Fat people are often the subject of undesired critiques of their bodies, typically said under the guise of “caring about their health.” No space may be more dangerous for fat individuals than healthcare, where weight is weaponized against patients by providers claiming to “do no harm.”
While the relationship between health and weight is tenuous, there is a clear relationship between anti-fat bias and adverse health outcomes, including increased stress levels and healthcare avoidance. When individuals seek care, the quality of care they receive is often lower. For example, when seeking cancer screening as a person who is fat, there are many barriers, including providers who will deny services such as a Pap smear based on weight. Additionally, there is a history of the medical system causing harm through the over-prioritization of weight loss. One such example is that of Fen-Phen, a combination weight-loss pill that was eventually recalled due to it causing valvular heart disease.
Increasing accessibility to genetic counseling for patients who are fat
Genetic counselors provide support for individuals navigating healthcare spaces. Even though someone’s weight is not the indication for an appointment, people who are fat do not come to us in a vacuum. Rather, we fit into their broader experience seeking healthcare, which often includes experiences of bias and stigmatization. We must understand these experiences to provide adequate support and mitigate additional harm.
Genetic counselors must examine how to make their practices more inclusive for fat people. Are the chairs narrow and with arms, which may be uncomfortable for someone who is fat? Is there utility in taking the weight of the patients you see for your appointment? How is weight used in cancer risk assessment models? Are you making assumptions about someone’s health-promoting behaviors based on their weight? How do you discuss healthy diet and exercise? How are you discussing and recording no-call cfDNA results, challenges with ultrasonography, or limitations of standard MRIs being able to accommodate some people’s body size?
We also must be mindful of our language. For many fat people, the common-in-healthcare descriptor of “obesity” often evokes a negative response and feels overly medicalized. The term obesity is also a direct reference to the Body Mass Index (BMI), an ineffective predictor of health with racist origins and uses. Similarly, avoiding the use of phrases such as “struggling with their weight” to describe people can help mitigate the idea that being fat is inherently something one struggles with.
For decades now, fears of the “obesity epidemic” have harmfully implied that a person’s fatness is inherently detrimental to society at large. Over time, these ideas become so ubiquitous that people rarely question them. As genetic counselors dedicated to providing unbiased and supportive care to all of our patients, we need to understand the importance of unlearning and reflecting on systems of oppression, and anti-fat bias must not be an exception.
Sarah Wiser, B.S. (she/her) is a second-year genetic counseling student at Boston University Chobanian & Avedisian School of Medicine. Sarah is passionate about promoting equitable access to genetic counseling services and challenging anti-fat bias in healthcare.
In his poem American Sonnet Billy Collins compares a sonnet to “furrows in a small, carefully plowed field.” Classical sonnets are tidily structured works that more or less follow a format of 14 lines, often in rhyme, the last two of which offer a resolution to the problem or question set forth in the earlier lines.* The strictures and structure of a sonnet and the image of a plowed and furrowed field makes me think of how genetic counselors try to neatly organize genetic counseling sessions. The templated counseling notes we produce afterwards – some version of Patient Identification, Medical History, Family History, Counseling Provided, Summary and Recommendations – reinforce the idea of a structured session as well as the sonnet metaphor.
We try to impose structure, for reasons both good and not so good. In many clinical positions, most patients are coming to us with a handful of similar indications such that we wind up saying more or less the same things over and over, especially when we carry large patient loads. My roteness would become clear to me when a patient “interrupted” me with a question about something else altogether and I would forget where I was in my game plan. I was not listening to the message the patient was sending – they were not much interested in what I was talking about and they wanted to discuss something more important to them. Genetic counselors, with our professional insecurities, also subconsciously want to impress others with our arcane knowledge and prove that we can make an important contribution to the health and medical care of patients and their families. This manifests itself most acutely during the early stages of a career, when we are still slightly unsure of ourselves and are trying to establish a firm professional footing and reputation. But even wise veterans can get caught up in this style, including and particularly me (well, not anymore, now that I’ve converted to my favorite religion – Reitrementism).
While acknowledging the important role that numbers and information play in genetic counseling and patient care, a counseling session is at its core a psychological interaction between human beings. It took me – no kidding – a couple thousand counseling sessions before I even started to become a good genetic counselor and adapted my counseling to the basic psychological truth that the human mind usually expresses its emotional self in a non-linear manner. I knew this on a cognitive level but it took me years to actually incorporate this insight into my practice. To paraphrase Maya Angelou, people won’t remember what you said but they will never forget how you made them feel.
What does this mean in actual genetic counseling practice? I’m not advocating for omitting facts and figures or abandoning an over-arching loose structure. A counseling session should have a beginning and ending, and complex biomedical information often needs to be imparted. You can start out with a highly flexible plan of issues and information you think should be covered while at the same time be very willing to modify the plan or abandon it altogether to meet the unique needs of each patient. It might begin with a query as to what the patient wants to get out of the session, though some patients are better at articulating that than others and some just aren’t sure of what they want. But however you start, you need to be prepared for traveling with the patient as they veer off in often unclear directions that are sometimes different than what the patient originally articulated. Structure, numbers, information – they are so comforting and comfortable to us, like Collins’ neatly furrowed fields. But the safe zone of an organized educational format can make us hesitant to explore the unplowed fields of the patient’s psyche.
What we can discover in those unfurrowed fields is what is important to patients, why it is important, and how it influences the way patients makes sense of complex biomedical information and what they should do with it. Fear of going through treatment for cancer after having watched their parent’s body ravaged by chemotherapy. Anger at an employer for creating an emotionally or physically toxic workspace and attributing their cardiomyopathy to this environment. A deep belief in “natural cures” that is being challenged by their lack of efficacy in treating their child’s illness. Feelings of abandonment and resentment toward a parent who died when the patient was an adolescent and who is now a parent of an adolescent themselves. Fear of having a child with a disability. A marriage adrift on two different seas. Distrust of medical practitioners stemming from having been treated disrespectfully in past encounters. All of the technical information can be so damn scary they don’t want to talk about recurrence risks or the chances of getting cancer or variants of uncertain significance, at least not right away and not by listening to what sound like a verbal spreadsheet. Genetic counseling is supposed to make the patient feel emotionally safe, not the counselor.
What this requires is actually attending to what the patient is saying or asking, especially if it has little to do with what you are discussing. You don’t want to briefly comment on what sounds like a non-sequitur from the patient and then return to the safety of your comfortable structure. Following the patient’s lead can result in a session which travels in several different seemingly unconnected directions (Why is the patient going off at this angle?), loops back on itself several times (Hmm, why does the patient keep coming back to that?), or has you probing the patient with questions neither of you had anticipated (“And so you’re saying MRIs are scary to you because you have claustrophobia and you’ve also read that the MRI’s magnetic field is thousands of times stronger than the earth’s magnetic field at its surface, and that’s why you are reluctant to undergo hereditary cancer testing?”). It can become a near stream of consciousness session that resembles James Joyce’s Ulysses more than Elizabeth Barrett Browning’s tenderly romantic How Do I Love Thee?. Joyce’s novel begins with the famous opening line that seems to presage a typical narrative – “Stately, plump Buck Mulligan came from the stairhead, bearing a bowl of lather on which a mirror and a razor lay crossed.” – then quickly changes tone and explores the depths of the minds of the novel’s characters and ends with Molly Bloom pouring out her innermost thoughts in an unpunctuated iambic-pentameter-be-damned eight sentence ~22,000 word uninhibited and unfiltered soliloquy. Kinda’ like a counseling session can go (Nothing against Barrett Browning. She is a marvelous poet; just a different style than Joyce’s).
I don’t know how AI chatbots will play out in the genetic counseling arena and how they might influence the structure of genetic counseling sessions. It seems possible that they might one day be capable of carrying out a psychologically sophisticated interaction with a patient that matches a counselor’s skill set as well as taking into account the patient’s socioeconomic situation, though I suspect not in the immediate future and hopefully not until the ethical issues have been addressed (for an amusing take on chatbots and genetic counselors, check out my post Genetic Counselor Reinvented). My bigger immediate concern is that administrators will simply see chatbots as a replacement for genetic counselors rather than as an ancillary tool for genetic counseling. Or that administrators will employ a strategy that employs both genetic counselors and chatbots but increases counselors’ patient loads on the premises that chatbots are doing a lot of the work and so you can fit more sessions into a counselor’s schedule. This ignores the emotional toll on genetic counselors who work with patients in stressful situations and will likely lead to counselor burnout and poorer quality patient care.
The potential and concerns about AI aside for now, the semi-chaotic session is often more valuable to patients than the biomedical lecture. Yeah, it can look and sound like a mess and be just as dense and difficult to understand as Ulysses. But that mess is where the beauty of the patient’s mind lies. Which is why we need to use our counseling skills to sort through the mess and understand the psychological meaning of the patient’s words, beliefs, actions, and choices. Hence the wonderful messiness of genetic counseling.
The Brain — is wider than the Sky — For — put them side by side — The one the other will contain With ease — and You — beside — by Emily Dickinson
Over the centuries, poets have played with the format of the sonnet to breathe new life into it, such as Wanda Coleman’s American Sonnet 91 and other of her decidedly non-linear poems that explore race and racism in America.
The single biggest problem in communication is the illusion that it has taken place. – Apocryphal quote, likely incorrectly attributed to George Bernard Shaw
A South Carolina court recently granted a summary judgment in favor of the defendant in the case of Williams v. Quest Diagnostics, Inc., Athena Diagnostics, Inc, ADI Diagnostics, Inc. The ruling is particularly relevant to the genetics profession because it concerns the potential legal implications of the classification of genetic variants.
This legal odyssey began nearly 5 years ago but the clinical story began 14 years ago, and was first reported here on The DNA Exchange. Briefly, Amy Williams, the plaintiff, filed a suit in 2016 on behalf of her deceased son alleging negligence on the part of Athena (now owned by Quest) when in 2007 it classified a variant in the SCN1A gene as a Variant of Uncertain Significance (VUS) in her son who had a seizure disorder. SCN1A pathogenic variants are diagnostic for Dravet syndrome.
Multiple specialists were involved in the child’s care, but it seems from the medical records that none of them were actually aware of the genetic test results. The ordering physician could not recall having seen the report and the treating physicians never received a copy of the report or a communication from the ordering physician about the result, even though a copy of the report is in the medical records. Consequently, her son’s treating physician kept him on carbamazepine, a sodium channel blocker that is contra-indicated in children with Dravet syndrome. Sadly, he died about 6 months later, likely due to the contraindicated medication. Ms. Williams did not find out about the SCN1A result until nearly 7 years after the report was issued, and then only after a genetic counselor who was sifting through the records found a note from 2008 referring to an SCN1A VUS (for a fuller description of this saga, I refer you to the excellent articles written by Turna Ray, a journalist for Genome Web).
The lab’s defense rested on a legal technicality of the statute of limitations. Per South Carolina law, litigation cannot be brought against a healthcare provider if the offense took place more than 3 years prior to the filing. The lab’s lawyers argued, and in 2018 the South Carolina Supreme Court agreed, that a lab qualifies as a healthcare provider under state law. Subsequently, Judge Margaret Seymour, the judge who presided over the original case (and who displayed an excellent grasp of the genetic and legal issues), found that several of the plaintiff’s claims were “comprised of allegations sounding in both medical malpractice and ordinary negligence” and allowed the matter to move to discovery for the purpose of determining what caused Athena’s laboratory staff to misclassify the gene variant. Ms. Williams and her lawyers proceeded with the case based on “claims for wrongful death, survival, negligent misrepresentation, constructive fraud, and violation of the South Carolina Unfair Trade Practices Act.” Following discovery, the defendants requested a summary judgment to dismiss the case (in a summary judgment, either a plaintiff or a defendant can assert that the facts in the case are not in question and ask the judge to make a decision on the case without a full trial).
Judge Seymour based her decision on the statute of limitations ruling by the South Carolina Supreme Court and the likely inability to prove proximate cause (i.e., that the VUS classification led to continued treatment with carbamazepine which then caused the child’s death), and dismissed the case: “The court concludes that no reasonable jury could find Defendants erred in classifying Decedent’s variant as a VUS, or that any misclassification was the result of nonmedical, administrative, ministerial, or routine care. Defendant’s motion for summary judgment is granted as to this issue.”
In an unfortunately cruel twist, Ms. Williams and her lawyers may owe Quest and its lawyers ~$140,000 in court sanctions imposed after some personal emails and other documents that, in my view likely had little bearing on the facts of the case, were deleted or improperly withheld because of less than stellar legal representation. The defendant’s lawyers offered to drop the costs stemming from sanctions if Ms. Williams agreed not to discuss the case in public forums and to discourage others from doing so. However, she did not agree to the proposal and remains firm in her belief that her son’s story needs to be discussed in public for the benefit of the public and the genetics profession, even in the face of potential financially ruin.
Was Athena’s original variant classification appropriate? Published case reports at the time the interpretation was first issued suggested that the SCN1A variant could be likely pathogenic (that was not the common terminology at the time), one of which was co-authored by Athena staff. Yet comments in the test report state there is an “absence of published studies correlating these variant(s) with clinical presentation and/or pathology.” In April of 2009, 2 years after the report was issued, Athena reclassified the variant as pathogenic, although they cited no new evidence beyond what was available when the report was first issued. Specialists in variant classification, who understand the intricacies of variant classification far better than I do, have weighed in and most have argued that Athena’s original classification of a VUS was appropriate for the knowledge available in 2007. Currently there are two entries for this variant in ClinVar, neither of which make an attempt at classification. I am not about to get into a debate with good scientists who know a heck of a lot more than I do about variant classification. I will say this, though, as someone who orders genetic testing every day, I rely heavily on labs to interpret variants and to let me know when there is in a result that might be grayer than ordinary. Especially in a case where a treatment decision with life and death implications hinges on a test result, I would expect the lab to explain their justification for the interpretation and to have made it clear in writing in the report. A phone call to the ordering provider wouldn’t hurt either, to be sure that the critical information and any uncertainty is clearly communicated.
Just as egregious, Ms. Williams should not have learned of a genetic test result almost 7 years after it was issued, and then only almost incidentally. Nor does it appear that the physicians who cared for the child were aware of the updated classification or communicated it to one another – not surprising, given that they were apparently unaware of the original report. Had she been notified in a timely manner, she may have initiated a discussion of why the variant was classified this way and if the evidence was strong enough to be the basis for treatment decisions. Of course this burden should not be on the patient but it could have offered another opportunity for further exploring treatment decisions based on the result. Many of us in the medical field, including me, have been critical of the requirement of the 21st Century CURES Act to notify patients of test results within 24 hours of when they are ready. My grumbling aside, Amy Williams and her son would have greatly benefited from being notified of her son’s result 24 hours after it were available. Does it have to take an Act of Congress to ensure that healthcare providers are responsible communicators with their patients?
In my view, nothing good came of this case in terms of the reputation of the genetics community, though of course nowhere near as bad as the devastating effects for Amy Williams and her son. To resurrect the line from the Captain’s speech in the movie “Cool Hand Luke“, what we have here is failure to communicate. Basically, a child may have died prematurely because of poor communication between the lab and care providers, between care providers, between care providers and the patient’s mother, and between the lab and the patient’s mother. Everybody lost and nobody won, even if Athena/Quest won from the perspective of not having to pay damages.
Will we now become better at communicating results to patients? Perhaps the CURES Act will help some. But as genetic testing expands well beyond the genetics community, communication about the implications of test results will likely still be deficient in many instances, in part because many non-specialists who order genetic tests are not particularly adept at interpreting them. Furthermore, although it’s hats’ off to ClinVar and other collaborative efforts for classify variants, variant classification will continue to be an Achilles’ heel of genome analysis because there is just no profit in it and it can be so damned complicated.
I look back on this story and feel a knot in my stomach.
The last decade has been boom times for genetic counselor employment. According to the 2020 NSGC Professional Status Survey (PSS), the number of genetic counseling jobs has doubled since 2010. Students are recruited for positions before they have graduated. The average starting salary for a genetic counselor right out of school is $12K a year greater than the entire profession’s average salary was in 2010. The highest salaries now exceed $200K. A genetic counselor with 5 years of experience can expect to make nearly as much as I do with 37 years of experience. If I were to go back to genetic counseling school and start my career a second time, I would probably be born again as a new counselor with a higher salary than what I currently earn (Hey Program Directors, think about what a headache it would be to have me in your next class!). And the 2020 PSS projected an even rosier outlook for the coming decade.
And then our parade got rained on by a storm of evil little droplets of RNA+protein. The US medical care system is facing the paradox of going broke while the urgent demands on medical services have never been more critical. By one prediction, the US health care system will lose two hundred billion dollars in the 4 month period from March to June. Those lap chole’s, knee and hip replacements, cardiac stents, and c-sections really drive hospitals’ bottom lines. It’s hard to believe that the rest of the year is going to look much better. I doubt that the US government will demonstrate the competence, unity, or interest to meaningfully mitigate the health care system’s financial woes, unless maybe New Zealand allows us to borrow Jacinda Ardern for at least 4 years.
It is not likely that genetic counselors will escape unscathed. So last week I informally surveyed the NSGC listservs (aka forums) about how the pandemic has impacted genetic counselors’ jobs. Here are a few replies about what some genetic counselors have experienced so far (anonymity preserved):
Partial furloughs
Lay-offs
Reduction in hours
Pay cuts
Reduction in non-salary benefits
Mandatory paid time off
Drops in referrals
Changes in job responsibilities from patient care to research and other duties
Job offerings withdrawn
It’s hard to know how prevalent these problems are because the “research” design and data have more limitations than a teenager who skipped school to go drinking with her boyfriend and wrecked her mother’s brand new car. But they do get your attention.
Like the virus itself, the impact on employment seems to hop, skip, and jump across the country. Some genetic counselors reported no effects at their institutions. To which I would add – at least, not yet. The health care system has just recently come up for air and many employers have not had the chance to fully assess the financial fallout. Early reports from well-respected commercial laboratories, who employ around 20% of genetic counselors, are worrisome too. Myriad reports that revenue has dropped 20-75% across its battery of tests.Invitae has seen testing volumes start to drop and has laid off some staff. These may very well be temporary setbacks and sales may rebound once the whole Covid thing cools off, whenever that might be. But they are not exactly encouraging signs. I am also curious to hear from our international colleagues about the pandemic’s impact on genetic counseling jobs outside of the US.
Once the worst of the pandemic is over, recovery is not likely to be a smooth and rapidly rising curve, even if – fingers crossed and offerings to St. Roch – the virus doesn’t return with a vengeance. Unemployment in general will be high and fewer people will have health insurance, and thus there will be fewer dollars to spend on medical care.
Christ Appointing Saint Roch as Patron Saint of Plague Victims, by Peter Paul Rubens.
Genetic counseling positions may not be high on the priority list of administrators if or when they look to restore lost positions in the future. In the grand tradition of administrators everywhere, they will look to cut costs and may replace only a portion of the lost genetic counseling positions. Hospitals and clinics may decide to shift genetic counseling responsibilities to other staff, such as medical assistants or nurse practitioners, or farm out genetic counseling positions to lab-based counselors, telehealth services, or even chatbots and videos. Older counselors may be nudged towards retirement. Expect paring back of support staff; executives always seem to forget that receptionists, schedulers, and the like are critical to running a hospital and cutting their salaries amounts to a hill of beans in overall budgets. Layoffs just about always come back to bite employers on the ass, and still they act surprised to find teeth marks on their buttocks.
The effects may even be felt in research funding. The NIH slated ten billion dollars for genetic research in 2020. Next year legislators and funding agencies may be more interested in diverting research funds to infectious disease research, prevention, and epidemiology. It’s hard to imagine someone running for political office on a platform of more money for genetics research and less for infectious disease research.
Oddly enough, current genetic counseling students may be better positioned than more experienced counselors. The salaries of genetic counselors with 5, 10, 20 years of experience can get pretty pricey for employers looking to save money. Why not hire somebody fresh out of school who would be paid a lower salary than a veteran?
I am not sure what the response of the profession can or should be. I think I have to leave that up to wiser minds than I possess. Perhaps the NSGC wants to start documenting the coronavirus job impact in a systematic way and plan a targeted PR push during the pandemic recovery focused on the value of genetic counselors in delivering health care. Training programs may think about scaling back admissions until the impact becomes clearer. Maybe the Accreditation Council for Genetic Counseling (ACGC) wants to slow down the approval of new programs. Genetic counselors may need to be more flexible about what they consider to be their scope of practiced and how genetic counseling services should be delivered.
Or maybe none of this will come to pass and by September we will resume our lives with some semblance of normalcy and a minimum of economic and existentialist wear and tear. I know I sound like Mr. Gloom and Doom, which is not really the voice you want to hear in these dire times. I understand why you might want to cover me in Greek fire, shoot me from a mangonel out and over the city walls, or disembowel me (my imagery is heavily influenced by a book I am reading about The Crusades, or as they are known in the Middle East, The Latin Invasions). So you can take heart in that fact that, like almost all predictions, there’s a pretty good chance I will be wrong yet one more time. But we shouldn’t stick our heads in the ground in an attempt to protect ourselves when the sky really is falling.
Lecturing patients is a lousy genetic counseling strategy. It presumes that the genetic counselor has superior knowledge and the respectful patient will listen to our learned words to make a perfectly logical decision about whatever it is they are seeing us about. But people don’t work like that, and while you are busy lecturing patients they are thinking about what to make for dinner that night, noticing the food stain on your shirt, or wondering if you will ever stop that incessant droning. Wise counselors instead prefer to reciprocally engage with patients and work together in symbiotic harmony to help the patient arrive at a cognitively and emotionally sound choice about whether to undergo a test, share information with family, undergo risk-reducing surgery, or whatever else is a critical issue for them. Victory all around; good counseling leading to good patient outcomes, and everyone is content.
Okay, so maybe genetic counseling doesn’t play out like that all the time. But it is a noble goal towards which we strive, however imperfectly.
You try to do your best to respect patients’ values and choices. Nonetheless, you can feel like a failure when a patient makes what appears to be a ridiculous decision. We’ve all been there, in its many permutations. The 55 year old BRCA1 pathogenic variant carrier who declines a risk-reducing saplingo-oophorectomy after she has tearfully confessed her deep-seated fear of ovarian cancer. The patient with a cardiomyopathy who has spent the last 30 minutes explaining that he wants testing so his young adult children can manage their risks accordingly – and then declines testing because he “doesn’t want to burden them with the knowledge.” The 33 year old, a mother of two young children, with newly diagnosed triple negative breast cancer who chooses treatment with antioxidant supplements and dietary changes over chemotherapy. Makes you want to pull your hair out (although seeking professional supervision might be a more fruitful pathway than self-inflicted alopecia).
Your first reaction is shock and disbelief. Huh? Was that patient in the same room as me? Did she not hear anything at all about what we discussed? Is she an idiot? I know you are not supposed to think that your patient is an idiot but sometimes those thoughts sneak in unbidden before your professional filter has a chance to block them. Hopefully that filter will kick in before you actually call the patient an idiot.
Or you may get defensive about it. Come on, lady, I know that I did a good job with you in there. I listened to you, we explored your thoughts together, I checked in regularly to make sure that you understood the key medical issues and how they impact your life. I validated and respected your feelings. I had the same interaction with my previous patient and she chose to have the surgery. How can you not uphold your end of the contract?
Mostly, though, such reactions reflect our personal and clinical insecurities. Any reflective counselor will – and should – have a healthy dose of insecurity and humility. Such seemingly outlandish decisions can be perceived as a threat to your professional ego and competence. What did I do wrong? Obi-Wan Counselor, my role model, would have handled this so much better. If she counseled her, that patient would definitely have chosen risk-reducing surgery. I am so incompetent. But I got news for you – there’s a darn good chance that Yoda-like role models still have many moments just like this. Perfect counselor no one is.
There could be several factors underlying what appears to be poor patient choices. Patients may be grappling with emotionally and technically complicated information that they just haven’t worked through yet and just choose something, anything, to get on with their lives for now. There may be a deeper psychological issue subconsciously driving patient choices, such as dealing with the long ago death of a loved one, confronting one’s own mortality, or fears of medical procedures because, when it comes down to it, who wants to be cut open. The expertise of a more skilled therapist may be required to address the situation.
Also, let’s face it, sometimes people just make dumb decisions, no matter how smart and psychologically together they are and how good your counseling skills are. We all do, at various times. Driving a car after wine and drinks with dinner, engaging in a flirtation or an affair when you are in a committed relationship, smoking cigarettes, crossing the street unsafely, spending money for an 18th pair of shoes when budgets are tight. There’s nothing too bright about any of those behaviors, although you have to be careful if you try to point out that a decision may not seem particularly good. It could alienate the patient, if not done just right. But I would argue that we all have a right to make what seem to be dumbass decisions.
Consider too that it is virtually impossible for anyone to know what will turn out to be a good decision. Any choice that tries to anticipate the future is so inherently complicated and filled with uncertainty that what seemed like a good idea at the time may eventually turn out to be an awful choice, and vice versa. All kinds of unanticipated outcomes or unknowable problems can arise. Serious complications might develop after risk-reducing surgery. Your beliefs, spirituality, perspective, and values may evolve over time. You had sworn off children and then you fall head over heels in love with someone and all of a sudden you want to start a family. You have a test for the sake of your family and then your family decides they really didn’t want the information and wish you hadn’t done it. You spend half your life worried about colon cancer and then you’re a victim of a pandemic. No one knows how the Cosmic Vanna White will spin her Rota Fortunae.
There’s no cookbook genetic counseling recipe that magically transforms people into rational and emotionally consistent decision makers. People are people in all their splendidly glorious contradictions and sometimes they are gonna’ do what they are gonna’ do. Sometimes we can guide them and sometimes we can’t. And sometimes, even when they don’t know it, they know what they are doing. Or they learn to live with their choices. That’s life and we can’t deny it.
In the United States, genetic counseling services are typically delivered by masters level genetic counselors. Yet Medicare, the largest health insurer in the US, does not recognize genetic counselors as reimbursable providers. No health professional is better qualified to provide genetic counseling than a genetic counselor. Absurdly, then, Medicare’s policy assures that the service is covered ONLY if it is provided by mostly unqualified health professionals. It boggles the mind.
But this could change if Congress passes H.R.3235 – the Access to Genetic Counselor Services Act, along with whatever version winds up in the Senate. This bipartisan bill would allow appropriately certified genetic counselors to be covered by Medicare and to order genetic tests as local licensure permits. The bill has broad support in the medical community. Even the AMA has stated they will not oppose the bill.
So why in God’s name has the American College of Medical Genetics and Genomics (ACMG), the primary professional organization of MD clinical geneticists, made the bone-headed decision to come out against this bill, even when many genetic counselors are members of ACMG? ACMG claims that they would support the bill only if genetic counselors are not allowed to order genetic tests. This is an untenable position, especially in light of the abundance of data demonstrating that genetic counselors not only are savvy about ordering tests but having them involved in the process results in significant cost-savings and increases the accuracy of test interpretation. I might add that there are virtually no equivalent data demonstrating that clinical geneticists bring equal value and expertise to the ordering and interpretation of genetic tests. They probably do but, hey, show me the numbers. Furthermore, the anti-genetic counselor position is contrary to ACMG’s Vision and Mission to “to facilitate the delivery of quality clinical and laboratory medical services to patients and their families…” It’s hard to facilitate testing if the country’s largest group of genetics providers are excluded from ordering genetic tests (there are roughly 2-3 times as many certified genetic counselors as there are certified clinical geneticists).
I suspect that ACMG’s position stems from both historical and economic factors. The relationship between masters level genetic counselors and clinical geneticists has a complicated 50 year history. When the first genetic counseling graduates entered the job market in the 1970s they were likely to be employed in a Medical Genetics department where they were supervised by a clinical geneticist. Not uncommonly, genetic counselors were viewed by clinical geneticists as lower echelon providers who more or less served as “doctors’ helpers.” Indeed, back then many clinical geneticists argued that genetic counselors shouldn’t even be allowed to call themselves genetic counselors because in their view only physicians should serve in that role. They wanted to wall off genetic counselors from meaningful clinical practice and call them Genetic Associates. There was also more than a hint of underlying sexism. Most clinical geneticists at the time were older males and 95% of genetic counselors were bright young females – those “girls” just weren’t good enough to do “real” medical genetics. The two professions, though, were in a symbiotic relationship; it would have been nearly impossible to run a large genetics clinic without the labor of genetic counselors or clinical geneticists. One profession could not live and thrive without the other.
With the wider availability of prenatal testing in the 1980s, many genetic counselors found employment in prenatal diagnosis clinics, which were usually run by obstetricians rather than clinical geneticists. Genetic counselors gained a greater sense of independence and professional confidence serving as the genetics experts in these new settings. This expansion of genetic counseling employment beyond traditional genetics clinics was further stimulated by advances in genetic testing for more common conditions like cancer and cardiac disorders in the 1990s. Genetic counselors were not gonna’ work on Maggie’s Farm no more whereas clinical geneticists pretty much kept themselves down on the farm.
As I have described previously, this came to a head in the early 1990s when the then American Board of Medical Genetics petitioned the American Board of Medical Specialties to create an American College of Medical Genetics. This move would serve to increase the prestige and potentially improve reimbursement of clinical geneticists’ services. The American Board of Medical Specialties agreed to do so – but only if masters level genetic counselors were not part of the deal. This resulted in very bitter debates between genetic counselors and clinical geneticists. I have vivid memories of some disagreeable and uncomfortable, uh, discussions at national and local meetings. One clinical geneticist told me at the time that the separation would mark the end of the genetic counseling profession (boy, was he wrong). Ultimately, with the thoughtful but firm guiding hand of the leaders of the National Society of Genetic Counselors, genetic counselors agreed to secede from ABMG. It turned out to be the best thing that ever happened to the genetic counseling profession. Genetic counselors and clinical geneticists thereafter still maintained a professional relationship; after all, many of them worked together. But professionally speaking, genetic counselors pretty much left clinical geneticists in the dust and clinical geneticists are still struggling to catch up. Most genetic counseling and ordering of genetic testing gets accomplished without any input from a clinical geneticist and it gets done quite well, thank you very much.
Incidentally, I would like to remind everyone that in the 1980s, when the American Board of Medical Genetics administered certification exams to both genetic counselors and clinical geneticists, all candidates need to pass two exams – a general exam that everyone took demonstrating overall knowledge of medical genetics and then a separate subspecialty exam each for genetic counselors and clinical geneticists. In most years that the exam was administered, genetic counselors had higher average scores and pass rates on the general exam than clinical geneticists did. So don’t talk to be me about questioning the competence of genetic counselors.
Economically, clinical geneticists are struggling to survive. Salaries are low and recruitment for fellowships is a struggle. Clinics are understaffed and wait times for an appointment in a genetics clinic can be as long as a year. Worse than running in place, they are losing ground. Thus, AMCG’s position on H.R.3235 gives the appearance of a desperate attempt to protect its shrinking economic and professional turf.
This is not 1980 and there aren’t any Genetic Associates anymore. Genetic counselors are damned good at providing genetic counseling and ordering and interpreting genetic testing. Genetic counselors know their limits; they aren’t looking to perform medical procedures, admit patients to hospitals, prescribe medications and other treatments, or undertake a comprehensive dysmorphology exam. In fact, in many states, local licensure laws already allow genetic counselors to order genetic tests if the patient has a private insurer or Medicaid (but not if the patient is covered by Medicare). I am not aware of any data suggesting that this has negatively affected the practice of clinical geneticists. It’s just made it easier for patients to access genetic testing, simplified navigation of the tortuous pathways patients must go through to obtain insurance coverage for testing, and helped assure that test results will be properly interpreted and integrated into the patient’s health care strategy.
But neither ACMG nor genetic counselors own genetic testing. Most clinicians, regardless of specialty, can order a genetic test. Heck, consumers can order tests themselves online, if they are so inclined. ACMG needs to better serve its membership and patients by adapting to a changing world and developing a different clinical and economic service delivery model. Opposition to H.R.3235 does not help patients, genetic counselors, or, if they cling to a dated view of medical practice, clinical geneticists themselves. ACMG must support H.R.3235 and recognize that genetic counselors play a critical role in the delivery of medical genetics services and testing.
You can contact your local congressional representative to express personal or organizational support fo H.R.3235.
Thanks again to Emily Singh for help with graphics.
I like doing crossword puzzles with their mix of trivia and clever word play. I will never win any contests, but I am a competent puzzler (I prefer the term puzzler to it’s more high falutin’ cousins, cruciverbalist and engimatologist). Sometimes a devilish clue will stump me because it leads my mind to a very narrow interpretation of it. I have found a helpful strategy to solving the clue is to give it some benign neglect. If I let my mind stray to other things and then come back to 23-Down, the cobwebs will have fallen and in a slap-the-forehead moment the answer pops into my head. One way of distracting myself is to let my eyes wander across the newspaper page. As it happens, crossword puzzles are often on or near the same page as Advice Columnists and I find myself reading those letters from people seeking help with their woeful life situations. I am usually impressed by the counseling and psychological insights offered by the columnists and often find myself wondering what my response would be to the letter-writers (and I find myself singing the lyrics to John Prine’s wry song “Dear Abby“).
Last Saturday when I was stuck on trying to remember the city where Aga Khan’s mausoleum is located, I turned to reading “Ask Amy,” Amy Dickinson’s advice column. Although Amy did not supply me with the answer to the puzzle clue (Aswan, along the Nile in Egypt, for those of you who are also puzzlers), my attention was grabbed by a letter to Amy from – a genetic counselor. The counselor, who has chosen not to have children, asked Amy how best to respond to clients’ questions about whether the counselor has children and what decision she would make for her own child. The counselor also related a story about a recent couple who believed that the quality of care provided by their physician was compromised by that provider being childless.
My first thought was “Such questions play on our professional and personal insecurities. This genetic counselor might have been better served by peer or one-on-one supervision.” Supervision is an important part of professional growth. Although there are a few genetic counseling supervision groups, they are not particularly common, perhaps because there is no strong genetic counselor cultural tradition for them or professional requirements to participate in one. To some extent, the NSGC sponsored listservs – or Forums, as they are now called – sometimes serve that role but it’s not exactly the same thing.
My second reaction was I guess that’s a question a chatbot wouldn’t have to deal with. As Siri might say, “I am not sure that I understand that question.”
My third thought was “What would I say to that counselor if she posed the question to me?” If you are in a clinical position, no doubt you have encountered similar questions about your personal life. Before I was married, I remember the not uncommon occurrence of counseling a single parent pregnant woman who came to the session with her mother and afterwards the mother asking me on the sly “You’re such a nice a young man. Are you married?”
It is impossible for us to mirror all of our clients’ characteristics, experiences, and life situations. We can’t be all things to all people. In fact, one might argue that being too similar to our clients can result in counter-transference issues that can negatively affect the quality of our counseling. A counselor can be too empathic; sometimes the ways that we are different from our clients can give us a less biased outlook on a family’s issues.
I was not particularly happy with Amy’s advice to the genetic counselor, which was to say to the couple “We’re not here to talk about me. We’re here to talk about you. Let’s focus on your case, OK?” I think it unhelpfully dismisses the couples’ concerns. It may be what the counselor is thinking but in my view that’s not how it should be verbalized or managed. I can think of a few alternative responses, depending upon the specifics of the situation:
“I appreciate your concerns and understand why you think a parental perspective might be helpful. But in my role with you, I am a counseling professional, not a parent. I have years of experience and professional training in working with couples in your position. My clients, whether or not they have children, often tell me how much they appreciate my expertise and insight. So I think that I can help you in meaningful ways. After meeting with me, you might want to talk to your friends and family members who have children to get their perspectives too.”
“You mentioned that you want your care providers to be parents – why do you think you feel this way? As we go through this session, let me know when you think a parental perspective would be important to the issue at hand and let’s see if we can figure out why my not being a parent might matter.”
“Some patients have raised this with me before. For many of them, it turned out that my perspective as a non-parent actually gave them a better understanding of their situation and helped them make what they felt to be a better decision. Let’s see if we can work together on this.”
“I don’t have children. But I listen very closely to my patients, and I have learned a lot from them about the issues and feelings that parents face. I think you can benefit from the many insights that my patients have shared with me.”
There are no doubt other ways to respond to these patient requests for self-disclosure and you may think my suggestions are inadequate. More than one research article has been written about how much counselors should share with patients about their professional lives and how they manage such questions. In the spirit of on-line peer supervision, I would like to hear from the Good Readers of The DNA Exchange about how they would have responded to the Ask Amy letter and how they handle questions from patients that probe counselors’ personal lives.
Patients are ongoing puzzles that we must continually work on solving, whether we are beginners or graying veterans. Some of the clues they give us have obvious answers, while others are more layered and complicated. The solution for one patient’s situation may not work for the next patient puzzle. All of us need to remain open to the help and perspectives of our peers and colleagues. We cannot grow if we engage in benign neglect.
Tala Berro is a genetic counselor in the Boston area. She is a queer, Arab woman who is also a racial justice and LGBTQIA+ activist. You can follow Tala on twitter here: @tala_berro
Bob Resta recently wrote a blog on his experience of being a man, as well as the advantages and disadvantages of being a woman, in our woman-dominated field. He called upon us good readers to share experiences “where you are not quite like everyone else.” Being a queer person of color in genetic counseling, I immediately took up his call. In part due to my various identities, there have been countless instances during my genetic counseling training and career when I have felt “not quite like everyone else.”
Let’s start with intersectionality, a term coined by Black feminist scholar Kimberlé Crenshaw in 1989 to highlight the ways in which black women were excluded from the feminist movement. Crenshaw notes that “not only are women of color in fact overlooked, but their exclusion is reinforced when white women speak for and as women.” In this blog post, I want to take a deeper dive into how my own intersecting identities as a queer, Arab woman affect my experience as a genetic counselor.
The genetic counseling profession within the Unites States is overwhelmingly white. As reported by the National Society of Genetic Counselors (NSGC), 92% of the 2018 Professional Status Survey respondents identified as white, which is easily visualized when one walks through the exhibit hall at the NSGC Annual Education Conference. Although there are many reasons why we often see a higher percentage of white individuals in jobs that require a graduate degree, genetic counseling is an especially white field. In comparison, 54% of software engineers are white, 80% of public school teachers are white , and 68.2% of physicians/surgeons are white.
The foundation of empathy is what drew me to the genetic counseling profession. I knew that I would come in as an outsider, but I hoped that caring, open-minded genetic counselors would make for caring, open-minded classmates, supervisors, and coworkers. However, we have a long way to go. Genetic counseling training programs incorporate lessons on the importance of culturally appropriate counseling of patients, but this same openness and acceptance is not always extended to fellow genetic counselors.
I started to notice my “otherness” in the field of genetic counseling from the beginning of graduate school. Being an Arab genetic counseling student always had its pros and cons. My favorite instances as a student were when an Arabic speaking patient would come into a genetic counseling session and I could utilize my knowledge of Arabic. This shared language and its ability to add comfort to my patient always felt really special. More often than not, though, sessions with Arab patients would end in a debriefing session with a supervisor who would ignorantly state microaggressions, judging family sizes, and gender dynamics. After one of these sessions, my supervisor and I were discussing the patient and mentioned the specific Arab country they were from. A medical professional in the workroom overheard and noted that, to her, this specific country is associated with danger and violence. There was no response to this comment. I was left shocked, dismayed, and anxious, without an outlet to seek support from other genetic counselors of color or Arab background.
What is currently seared into my mind as a genetic counselor of Arab descent whose community often attends mosque, is the massacre in New Zealand. I came to work devastated and shaken. While not all individuals of Arab descent are Muslim, I (and many others) consider those who are Muslim to be members of my community. Perhaps a genetic counselor saw a Muslim patient that Friday and provided comforting words. I wondered, though, how many genetic counselors reached out to their peers or students who may have been impacted by this. From my own experience of not receiving messages of support, I would guess not many.
In addition to racial barriers, being a queer genetic counselor comes with its own barriers to navigate. Based on my training experience, genetic counselors are growing in their awareness of pronouns and gender identity, often using the word “partner” when counseling. However, on an interpersonal level, it takes more than just awareness for true inclusion. I recall a conversation from back when I first started as a genetic counseling student in which I proudly identified myself as queer. This statement was met with discomfort and confusion. I know that genetic counselors are educated on the importance of mindfulness and inclusivity of the LGBTQIA+ community and are taught to be verbally-inclusive with patients who identify this way during a session. However, there seems to be a discrepancy in how these lessons of acceptance are actively applied by genetic counselors in and out of clinic. The ability to sustain a relationship with a patient over a 60-minute genetic counseling session does not translate to intentionally cultivating an authentic relationship with someone of a different identity from you.
One universally challenging aspect of genetic counseling training is providing and receiving feedback. To be evaluated on your words, demeanor, and body language while you are learning to interact with patients and cope with emotional situations is difficult. However, feeling like you are also being evaluated for your values, beliefs, and cultural upbringing is much harder. At times, I have been critiqued for my character and values, as opposed to my specific counseling skills. I have been encouraged to “play devil’s advocate” to my own beliefs. For example, during my training, I was given feedback that highlighted my potential to advocate for underserved patient populations, and also challenged me to find ways of connecting with patients who are different from me. This feedback came before I even had the opportunity to interact with a single patient. I felt critiqued not on behaviors I exhibited but on behaviors that were assumed of me. It also felt like this feedback was unnecessary reiteration that I am different, as the minority, and that I will be expected to live and fit in a world of the majority. Through these experiences I wondered: were my professors and supervisors feeling defensive because I was different from them and teaching me felt different than teaching others in our field? Who could I turn to within the field to talk about my thoughts and concerns?
Whenever I hear the term devil’s advocate, I think back on a blog post by Juliana Britto Schwartz. She writes, “dearest devil’s advocates: speak for yourself, not for the ‘devil’. Teach yourself. Consider that people have been advocating for your cause for centuries, so take a seat. It’s our time to be heard.” It is often forgotten that those with underrepresented identities have lived their entire lives being forced to understand the majority. These same privileged experiences to which I was encouraged to have an open mind are mirrored by what I read about in fiction, watch on television, and learn about in the history books. As a queer genetic counselor of color, I understand how to navigate these spaces because I have been forced to my whole life and will continue to do so in my professional life. Instead of ensuring that I understand and empathize with the majority experience, why don’t we make sure that the majority understands and empathizes with the minority experience?
As genetic counselors, we consistently discuss and learn about empathy for our patients. My hope is that we can take these lessons and apply them to our colleagues and peers outside of a counseling session. To my fellow genetic counselors, I propose the following version of the golden rule: treat your peers as you treat your patients.





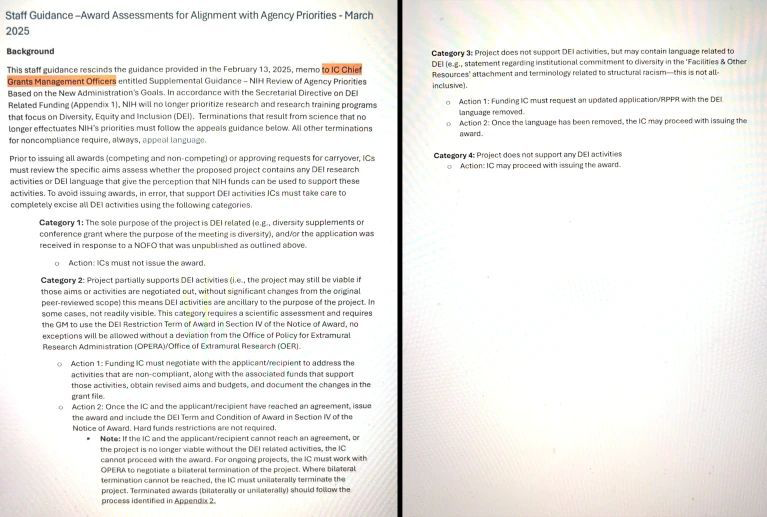














{kind=link}