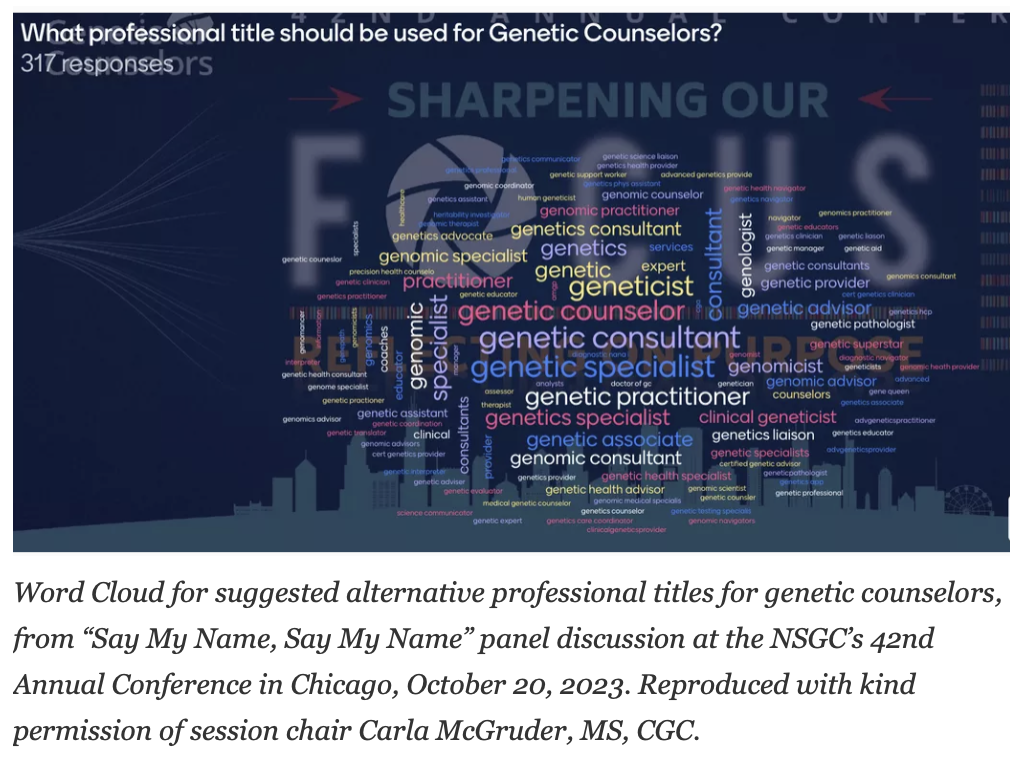
At the recent annual conference for the National Society of Genetic Counselors (NSGC) in Chicago, there was a spirited debate about whether or not to change the genetic counselor name. An alternate name was not presented, but below is a word cloud of proposed alternate names which DNA Exchange author Bob Resta shared in his recent blog post, where he decided to decline supporting a name change.
An informal poll that was circulated after the debate found that a significant percentage of genetic counselors were also wary of pursuing a name change.
For those who have not seen the debate, there were two primary tensions between the “pro change” side and the “pro same” side. The “pro change” side argued that changing our profession’s name could bolster NSGCs Justice, Equity, Diversity and Inclusion (J.E.D.I.) action plan (https://www.nsgc.org/JEDI), theorizing that possibly one of the reasons that genetic counseling is less diverse than many other professions is that our name creates a branding and recruitment problem. The “pro same” side brought up that if we genetic counselors change our name, then we’d need to update all of our state licenses, plus the language in our pending legislation to have Medicare recognize genetic counselors. Mr. Resta agreed that these issues were also an important factor to consider. The pro-same side also brought up that Physician Assistants are currently changing their name to Physician Associate, and that the associated cost of their name change is estimated at approximately $22 million, which would obviously be a staggering expenditure for an organization like NSGC.
Looking further at the “pro change” perspective, NSGC has rightly committed itself to implementing a successful J.E.D.I. Action Plan. Diverse teams provide better clinical care, better research, and build better businesses, all sectors where genetic counselors commonly contribute. Competing for diverse talent is in many ways the competition for the future. In a white paper published by the consultancy McKinsey in 2020, titled “Diversity Wins: How Inclusion Matters,” they outline the many ways that more gender and racially diverse organizations consistently outperform their less diverse competition, and argue for a greater focus on multivariate diversity (meaning “going beyond gender and ethnicity”). Currently, genetic counseling is among the least ethnically diverse fields in healthcare. We genetic counselors have an enormous amount to gain from a successful J.E.D.I. initiative. Over the long-term, perhaps far more than $22 million worth of benefit, if such a thing could be calculated. So, if strong evidence emerged that changing our name would substantially improve NSGCs odds of a successful J.E.D.I. program, then it’s prudent to consider this option with an open mind. We can’t just say that we’ll implement a J.E.D.I. program “unless it’s challenging or expensive,” right? If NSGCs J.E.D.I. initiative is a priority, then we should prioritize it. And maybe, there isn’t as much sacrifice as the “pro same” side implies.
Let’s also assess the state licensure argument more closely. There are lots of state licenses for all sorts of fields (see here and here for more info). Millions of people have state licenses all over the United States, including licenses for athletic trainers, auctioneers, and barbers, to name a few. So as a political matter, getting a state government to issue a professional license is often a manageable process. That’s why NSGC has approximately 35 state licenses. Importantly, a name change is drastically easier to navigate through a legislative body than a whole new license. Legislative bodies often use a “consent agenda” to take care of matters that are considered “technical and non-controversial.” It’s hard to imagine a piece of legislation that is more “technical and non-controversial” than changing the name on the genetic counselor license, as long as we don’t trigger a turf war by calling ourselves something like “doctor” or “geneticist.” In some states, we might even be able to get a name change done with volunteers, no lobbyists needed. And even in the states where we would need lobbyists and perhaps the consent agenda isn’t an option, this should not represent particularly expensive lobbying. If we genetic counselors decided to change our name, it would indeed require volunteer work to amend our state licenses, and it would have associated financial costs, but this is hardly an insurmountable hurdle – and one well worth jumping over to accomplish NSGCs Justice, Equity, Diversity, and Inclusion goals.
Next, let’s investigate the argument that a name change could hamper our efforts on Medicare recognition. Medicare is a massive and expensive federal program, and while there are different ways to calculate it, many legislators believe that recognizing a new provider, such as a genetic counselor, would represent a cost to a program that is already too expensive. So, unlike a state license, getting the United States Congress to recognize a new provider under Medicare is politically extremely difficult. In fact, after nearly two decades of effort, NSGC still hasn’t made any substantial progress on Medicare recognition, which in the context of this debate (and really only in the context of this debate), is actually a good thing. We haven’t even made it through the House or Senate. So, our lack of Medicare recognition at the present time argues in favor of exploring a name change, not the other way around, since our bill is still going through a process where amendments are common anyway.
To summarize, the benefits and costs of changing the genetic counselor title have not yet been fully flushed out. The debate at NSGC, while very thought provoking, was a starting-off point. We need to identify the best contender for an alternate name, and assess the benefits the alternate name is likely to generate. Perhaps the right name could both bolster the J.E.D.I. action plan and improve our prospects of gaining Medicare recognition, by better succinctly representing a genetic counselor’s value to the healthcare system. In parallel, we need to understand what the costs would be specifically for genetic counselors, as opposed to using Physician Assistants (I mean, Associates) as a proxy. PAs can already bill Medicare, have a different scope of practice, there are about 150 thousand of them in the United States, and there are likely many other differences. While their experience is of course informative, they are not a reasonable proxy. Once we have a better sense of what a name change would mean specifically for genetic counselors, then we can weigh the estimated benefits of the identified new name against the estimated costs. Importantly, when assessing the costs, we shouldn’t only ask lobbyists who expect to bill us for their services, as they have an obvious financial conflict of interest.
A successful J.E.D.I. program was always going to require substantial work, cost money, require new ideas, and require openness to meaningful change. Changing the genetic counselor name would indeed require NSGCs political operation to put in effort, but what is the point of having a political operation if we’re afraid to interface with the political system? If we can’t identify a new name that would propel NSGC’s J.E.D.I program, then it’s not worth the cost and effort. But I strongly support researching a new name further, and politically speaking, if we can’t handle a name change to a state license, then we can’t handle much of anything. And a name change may be easier than Mr. Resta’s charming idea that we convince George Clooney and a major network to launch a TV show about genetic counselors that’s as successful as the Sopranos.
There’s a lot of tricky questions that arise that aren’t touched on in this piece. A name change would need to be a slow and thoughtfully planned process – staffing, volunteers, timing, budgets, and not to mention the new name itself. There are likely other costs that haven’t been identified yet. We might not even like the new name, but remember, it’s not for the majority of current genetic counselors – it’s for the future of genetic counseling.
Misha Rashkin has been a genetic counselor for 10 years. He is a clinician and specializes in oncology. He has a longstanding interest in the ethical and legal issues of genetic testing, particularly the Genetic Information Non-discrimination Act (GINA).
At the recent NSGC Annual Conference, Carla McGruder chaired a sparkling plenary session titled “Say My Name, Say My Name”during which panelists debated the pros and cons of the professional title Genetic Counselor (there was widespread disappointment that Beyoncé did not make a guest appearance). The general sense I got from the debate was that there was enthusiasm for a name change and that a new professional title may ultimately prove to be destiny’s child, but for now no one offered a particularly winning alternative (see below word cloud from the session). Perhaps unsurprisingly, nobody brought up my two biggest long-standing concerns about the genetic counselor title. One is that the oft-used abbreviation of GC for genetic counselor is also the abbreviation used for gonococcus bacteria (though then again it could also more appropriately suggest guanine and cytosine). My other concern is that we should more properly be called genetics counselors; genetic counselor without the “s” at the end of genetic makes it sound like being a counselor is a hereditary condition, the result of some likely pathologic variant. I am pretty sure, too, that lots of genetic counselors in Canada, the UK, Australia, and some other countries would prefer everyone spell it “genetic counsellor.”
Word Cloud for suggested alternative professional titles for genetic counselors, from “Say My Name, Say My Name” panel discussion at the NSGC’s 42nd Annual Conference in Chicago, October 20, 2023. Reproduced with kind permission of session chair Carla McGruder, MS, CGC.
Debate about what to call ourselves has surfaced with some regularity since the profession was birthed a half-century ago at Sarah Lawrence College, and in a journal article by Jehannine Austin and their group at the University of British Columbia, as well as being the subject of two prior DNA Exchange postings, one by my DNA Exchange colleague Allie Janson Hazell and one by me. I suspect that currently the name debate is driven by the profession’s expansion into so many new employment niches, many of which do not involve direct patient care. It may also be influenced by the increasing trend of the profession defining itself – and being defined by other health professionals – in relation to genetic testing.
Let me state my biases up front. I am opposed to a name change, at least until you can show me something better that will justify the very extensive, expensive, and intensive efforts of introducing a new name and eliminating an old one. Of course, my biases are partially driven by being an Old School GC, having graduated in the Late Neolithic Period of genetic counseling, back in 1983. There’s always the attitude of “Damn it, the way I was taught is the right way.” And even if someone comes up with a better job title, I will still likely go to my grave calling myself a genetic counselor. But my personal hang-ups and emotional reactions aside, let’s take a look at some of the pro arguments and why I think they fall short.
One of the pro arguments for a name change centers on lack of public awareness of just what a genetic counselor is or does. Yeah don’t we all know that one! I can’t disagree with this point. But changing our name will not in and of itself improve public awareness or visibility. The alternative names are equally or more ambiguous. Patients will probably react with uncertainty to titles that include the likes of analyst or consultant or specialist (to name just three) and it will do nothing to clarify how we might help and serve them.
While acknowledging the general lack of public knowledge about genetic counselors, we have nonetheless made remarkable progress in increasing awareness of the job title, both with patients and healthcare providers. The below Google Ngram, with all of its limitations, gives a rough idea of how much awareness of genetic counselors has increased since Sheldon Reed christened us in the 1940s, with the ambiguous but reasonably accurate definition of “a kind of genetic social work.” A lot of that progress can get lost if you eliminate the genetic counselor title.
If you really want to improve public awareness, you have to think beyond name changes and PR campaigns. Look at what the Dr. Jennifer Melfi character in The Sopranos did for publicity for therapists. What we need is a successful streaming series about genetic counselors, complete with gratuitous sex and nudity (we can hold off on the violence; there’s more than enough of that to go around in the world these days). I can picture the genetic counseling show’s log line: “Family Lines” – Follow the professional challenges, joys, tragedies, and dilemmas as well as the complicated personal lives of young, attractive, ethnically and gender-diverse genetic counselors as they graduate from their training programs and experience the impact of genetic conditions on their patient’s lives and families as well as on the counselors’ own psyches. Starring George Clooney as the dashing veteran Robert “Bob” Resta whose efforts to guide this gaggle of counselors throughout their careers are undermined by his own very human failings.Consider running the credits over a background of a pedigree being drawn to highlight the commonly used genetic counseling tool and to evoke the name of the show.
Proponents of a name change quite rightly claim that the term “counselor” doesn’t reflect what many genetic counselors actually do in their day-to-day work. Genetic Counselor does not capture the essence of a Variant Analyst, Professional Support Specialist, Product Development Manager, Program Administrator, Researcher, or Medical Science Liaison. But, according to the 2023 NSGC Professional Status Survey, 71% of genetic counselors are involved with full or part-time direct patient care. This suggests that a significant majority of us are actively engaged in genetic counseling on a regular basis, so it makes sense to call us genetic counselors.
Besides, the proposed alternatives capture an even smaller range of what genetic counselors do for a living or otherwise sell our skill set short. For example, one of the suggested alternatives is something along the lines of Genetic or Genomic Information Specialist. It strikes me that the word “Information” misses a critical insight into the human psyche. It isn’t so much the information that’s communicated that is key as it is the way that each person’s mind uniquely interprets that information and integrates it into their lives. this is where counseling skills come in, which, for my money, is what sets the profession apart and makes it uniquely valuable. It gives us a professional identity unlike any other genetics profession or specialty. The value of counseling and communication skills is acknowledged by many genetic counselors employed in non-direct patient care positions, who often claim that their counseling and communication skills have been key in enabling them to expand into their new roles. They are still using basic genetic counseling skills, just in a different context.
Furthermore, I would argue that the very ambiguity inherent in the genetic counseling title is what has allowed us to grow our professional roles. Other professional titles might not provide the flexibility to expand into new and exciting roles. If employers are not exactly sure of what we do, it allows us create new roles that other providers don’t have the knowledge base or skill set to match. As Ed Kloza – who has pretty much witnessed the entire history of the profession first hand – sagely pointed out at the microphone at the “Say My Name, Say My Name” session, the title genetic counselor has gotten us pretty far professionally since the 1970s. Just how has it limited us?
A decidedly practical drawback to changing our professional title lies in the bureaucratic underpinnings necessary to maintain the life of a profession. It’s not just a name that can simply be eliminated by a search-and-replace function. The title Genetic Counselor is written into state licensure laws, pending federal legislation to make genetic counselors recognized Medicare providers in the US, and other countries’ equivalents of licensure. To say nothing of changing job titles by every employer of genetic counselors, the names of a half dozen or so professional organizations, a journal title, and a PubMed search term, to name a few. This could potentially be achieved but you need a very, very compelling reason to expend all that energy, time, and money doing so.
It will be interesting to see what what happens with the job title in countries where the genetic counseling profession is just establishing itself – such as India, the Philippines, and the Middle East. Local circumstances, medical practice, and cultural preferences may wind up generating some very different names and professional practices. But I suspect that they may also want to stick with the genetic counselor title to capitalize on the remarkable progress the profession has made in the US, the UK, Canada, Australia, and elsewhere. The practice and profession may look a bit different around the globe, but they will still be recognizable as genetic counselors and not as something else.
Perhaps too, it is time to reconsider the 2006 standard definition of genetic counseling. While I happen to be a champion of that definition, my professional conflict of interest is that I helped craft it. The current generation of genetic counselors should not necessarily have to rely on a definition created by a previous generation if it no longer captures the essence of genetic counseling. This could have bearing on whether we should choose a new professional title.
For now, though, Genetic Counselor may be a less than perfect name but it is closer to perfect than the proposed alternatives. Give me powerful reasons to think otherwise, and I will change my mind. Until then – Change my name? Nah.
What is the economic worth of one person’s life? That question was raised yet again in a recent paper on expanded carrier screening (ECS) that justified an expanded carrier panel based on the cost-savings garnered by avoiding the birth of people with any of 300 mendelian disorders. A quick and likely incomplete literature search revealed other similar publications from around the globe (Azimi et al., 2016; Beauchamp et al., 2018; Busnelli et al. 2022; Clarke, 2021; Wang et al., 2022). NSGC’s Expanded Carrier Screening Guidelines also point to economic gains as one of the benefits of carrier screening. Other professional guidelines and research papers do not discuss the economic benefits of expanded carrier screening, though read carefully, the disability avoidance/cost savings theme is often an undercurrent. To me, economic justifications for ECS raise serious concerns.
The quantification of saved costs over time will help to critically examine the medical necessity of ECS as a proactive health screening strategy. – NSGC Expanded Carrier Screening Guidelines,2023
To be clear, I don’t object to carrier screening per se and a “pan-ethnic” panel can make more sense than an ethnic-focused panel. All patients deserve the right to make complicated and highly situated reproductive decisions and access to genetic testing should be fair and equitable, points which most professional guidelines agree on. My concerns arise from the purported economic benefits of ECS through disability avoidance (I, along with Katie Stoll, have some other concerns about ECS besides economic cost benefit analysis).
But first some historical context.
During medical genetics formative decades in the mid-20th century, the concept of cost-savings by preventing the birth of people with genetic conditions was baked into the field, using ingredients leftover from eugenics. Many leading geneticists at the time preached about the economic and other costs to society of genetic mutations (and by extension, the worth of people who carry such pathologic gene variants), and how it was important to eliminate these pathologic variants to save society money and to preserve the future of humanity itself. While post-World War II geneticists typically disavowed old school eugenics, many of their concerns continued to echo the field’s eugenic origins.
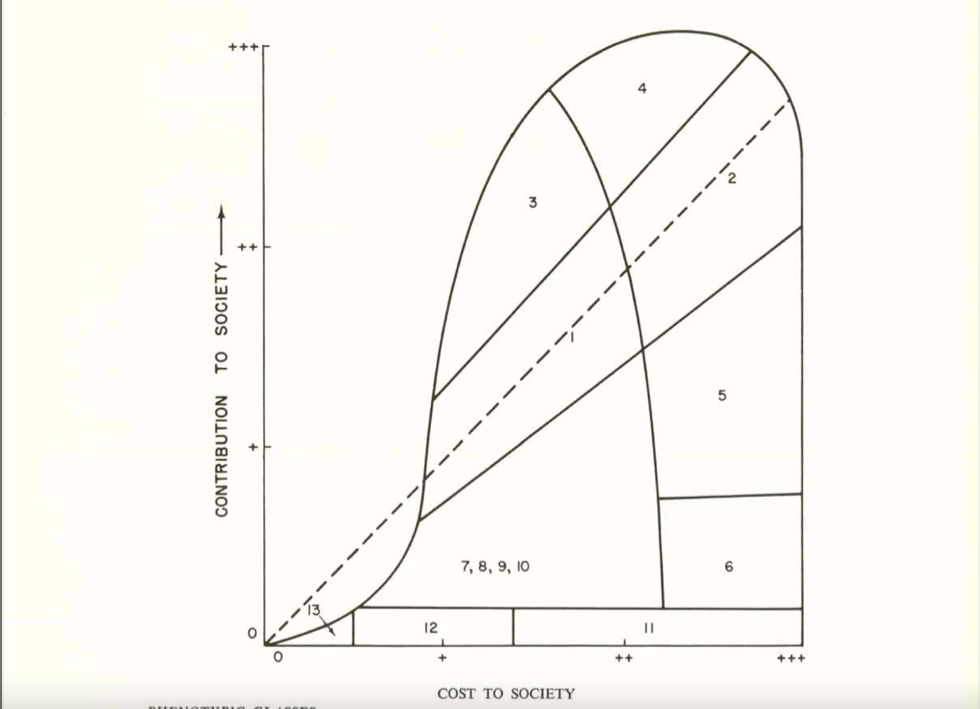
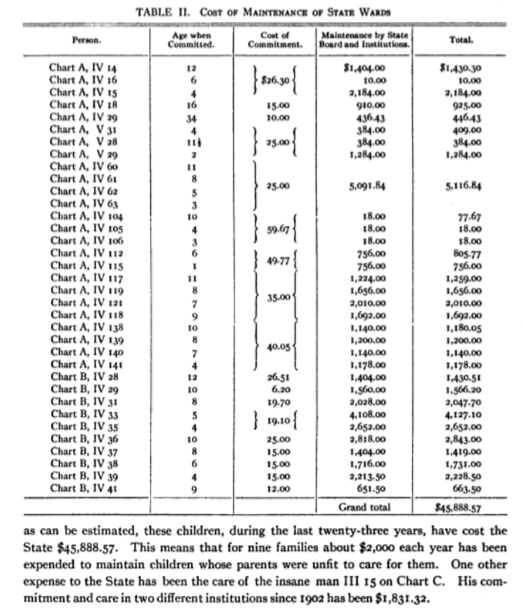
Let me illustrate this history with a notable example. In 1954, the National Academy of Sciences formed a group called The Committees on The Biological Effects of Atomic Radiation (often called The BEAR Committee), six separate committees that were charged with reviewing the available data on the range of biological effects of atomic radiation. A 1960 report from this group detailed the findings from the Committee on Genetic Effects of Atomic Radiation. The genetics committee was comprised of some of the leading brilliant geneticists of the day – George Beadle, Bentley Glass, James Crow, Theodosius Dobzhansky, Herman Muller, James Neel, and Sewall Wright, to name a few. Sewall Wright, in his chapter in the report “On the Appraisal of Genetic Effects of Radiation in Man,” divides humanity into 13 groups, based on intellectual, behavioral, and physical traits. Wright then decides the degree to which each category’s contribution to society is greater or lesser than its cost (as far as I can tell, based on Wright’s opinion and zero data). Some examples of these categories give an idea of their flavor:
1. In the first category, which includes the buIk of the population, there is an approximate balance between contribution and cost, but both at relatively modestlevels.
4. In this category are those who cost society much in term of education and standard of living but who contribute much more than the average at their level of cost.
6. We may put here individuals of normal physical and mental capacity whose cost to society outweighs their contribution because of the antisocial character of their efforts: charlatans, political demagogs, criminals, etc.
8. Low mentaIity but not complete helplessness.
10. Mental breakdown after maturity, especially from one of the major psychoses.
Sewall Wright, great statistician that he was, then graphed out these categories in this figure:
People in categories above the dashed midline contributed more to society than they cost, for people in categories close to the midline their cost/benefit was a wash, and people below the midline cost more than they contributed. In Wright’s view (and presumably the view of most of the genetics committee), anybody in Categories 7 or below cost more to society than they were worth. Oddly, those in Categories 5 and 6, were “acceptable” to Wright, even though their cost to society were greater than their contributions. He may have had a soft spot for playboy types, charlatans, and criminals, although he was also unsure of the genetic contribution to these traits .
Wright’s graph did not go unnoticed. Victor McKusick, whose obituary called him “The Father of Medical Genetics,” reproduced Wright’s graph in his 1964 short book Human Genetics, one of the earliest modern medical genetics texts. On page 141 of McKusick’s text, he goes on to say “No one would dispute the desirability and scientific soundness of encouraging reproduction of intelligent persons who are an asset to society.” And it didn’t end there. Cost effectiveness studies continued to be raised to justify the introduction of heterozygote carrier screening and amniocentesis in the 1970s and beyond.
From an ethical perspective, I find it appalling that the cost-savings to society is hailed as a benefit of expanded carrier screening. Do we really measure the worth of a human life by how much money they contribute or cost to society? Isn’t that whatpeople with disabilities, their supporters, their families, and disability scholars have been screaming at us for like a million years? Are we that tone deaf that we can’t hear their shouting? Are we just pretending to hear them or are we simply ignoring them? Isn’t a human being’s worth measured by non-economic factors? Who’s to say whose life is more worthwhile than others or how it should be measured? Why is it that people born with a genetic condition are less valued than people who develop disorders after birth that are even more economically burdensome, like dementia, lung cancer, diabetes, and heart disease (the risks for many of which can be reduced by low cost interventions like improving diet and exercise, and avoiding tobacco and excessive alcohol intake)?
Cost-savings justifications are also incompatible with Diversity, Equity, Inclusiveness, and Justice (DEIJ) initiatives. Money-saving justifications imply that if you are born with a genetic condition and cost society too much money, we are not going to include you. The message is that we support DEIJ for the “right” kind of people, those whose genomes and phenotypes aren’t too costly.
From a technical standpoint, many cost-effectiveness studies suffer from some serious flaws. For example, the Beauchamp et al. paper mentioned above includes 176 conditions in their analysis. Realistically, and which the authors acknowledge, there is no way to obtain reliable lifetime costs of all 176 conditions, given the rarity and variable prognosis of most of them. Also, the greatest economic cost benefit comes from the conditions associated with increased likelihood of survival to adulthood and the attendant need for ongoing care, such as Fabry disease, cystic fibrosis, the hemoglobin disorders, and Wilson disease. Adding on dozens and dozens of other uncommon conditions, often associated with early death, does not add much to the economic savings (a point also made in the paper by Azimi et al., cited above).
Cost-savings studies also often make the erroneous assumption that people who have a genetic condition make little or no economic contributions to society. Tell that to all the hard-working adults with Fabry disease, cystic fibrosis, deafness, hemoglobinopathies, etc. Not to mention the many non-economic benefits that any individual – regardless of their genome or phenotype – may “contribute” to society, such as joy, love, friendship, community, artistic creativity, etc.
But you might argue that health resources are limited and saving billions of dollars can’t be ignored, whatever the exact amount. That saved money could go to treating people with genetic conditions. Well, first off, there is no reason to believe that such abstractly saved money would be funneled directly into the care of patients with genetic conditions, or for that matter back into the health care system itself. The theoretically saved money could just as easily wind up funding some legislator’s pet project.
Furthermore, the savings are not quite as impressive as they sound. For arguments sake, let’s accept the estimates of Beauchamp et al. that on average each condition incurs a lifetime cost of $1.1 million (US) and that 290 of every 100,000 pregnancies are affected by one or more of these 176 conditions. Assuming about 3.6 million births in the US each year, that would result in 10,440 children with one of the screened conditions. At a lifetime cost of $1.1 million each, that adds up to ~$11.5 billion in savings over their lifespan (I am making a “best” case but unrealistic assumption that all at risk couples are identified and all affected births are avoided by preimplantation genetic testing, prenatal testing and termination, avoiding reproduction, gamete donation, etc. Cost-effectiveness studies of course don’t make such unrealistic assumptions).
On the other hand, the annual (not lifetime) spending on all health care in the US is $4.3 trillion, per the Center for Medicare & Medicaid Services. The lifetime costs of caring for people with the conditions included in an expanded carrier screening panel is barely a rounding error in annual health care spending in the US. Is the purported savings benefits of expanded carrier screening worth a rounding error, in light of its ethical shortcomings?
Figures 2a and 2b from the Beauchamp et al. reference cited above, illustrating the cost-effectiveness of different carrier screening strategies. Note how the graphs visually evoke the Sewall Wright graph above.
Another justification offered for ECS is the claim that money is saved by shortening the diagnostic odyssey and thus reducing visits to specialists and avoiding unnecessary and inappropriate treatment and testing. Certainly shortening the diagnostic odyssey is a laudable and important goal. However, cost calculations based on that claim are likely to be flawed. We don’t know how many babies born with the screened conditions would experience a diagnostic odyssey, how long the odyssey would take for each condition, and how much unnecessary spending would have been avoided. Nor do we really understand how many children undergo the diagnostic odyssey overall or what percentage of these journeys might be avoided by expanded carrier screening. Besides, the diagnostic odyssey could be more effectively shortened – though by no means eliminated – by expanding newborn screening and/or improving the availability of, and access to, whole genome sequencing, which would allow diagnosis of a much broader range of conditions than those included on carrier screening panels.
A potential and subtle danger of emphasizing the economic benefit of ECS lies in the absurd economics of healthcare that results in the high cost of new and innovative ways of treating genetic disease based on the underlying pathologic variant. Delandistrogene moxeparvovec-rokl (Elevidys), an anti-sense oligonucleotide (ASO) for approved by FDA in June for treating Duchenne muscular dystrophy patients with certain dystrophin variants, is priced at $3.2 million (US). As pointed out by Dan Meadows in this space a few weeks ago, the cost of nusinersen (Spinraza), another ASO, to treat some forms of spinal muscular atrophy, is estimated to cost ~$750,000 (US) the first year and $375,000 per year thereafter. Such high costs of treatment further bolster the belief that treating genetic disease is too costly. Paradoxically, just as at least partially successful treatments are finally becoming available for some genetic conditions, there may be a move to further prevent more births of people with certain genetic conditions in order to save money.
It’s tempting to equate cost-savings with eugenics. However, I think the eugenics label adds nothing to the discussion, other than being an accusation that turns the discussion into an argument. Whether or not it’s eugenic depends on how you define eugenics, and there is no widely agreed on definition. I think it is inaccurate to broadly label medical genetics and genetic counseling as modern day eugenics. Nonetheless, arguments for cost savings and disability prevention betrays the field’s eugenic roots and how we have not fully come to grips with our history. The graphs and table displayed in this post are not exactly the same, but they do share a pedigree. With each generation, the graphs and tables change to reflect their times, but the underlying message remains constant.
Medical geneticists and genetic counselors are not an unethical bunch. In fact, I have always been impressed with how much we struggle with complex ethical issues on a daily basis. But our vision can be subtly influenced by our history and by the fact that many – probably most – clinical and laboratory positions rely on the availability of genetic testing. We try to so hard to be good but sometimes it blinds us to the bad we might do. As Devin Shuman so elegantly reminded us in this space last week, the good intentions of our ableist assumptions can do a lot of harm. It’s about time we shed the ethical baggage of economic savings based on avoiding the birth of people with disabilities.
This month is the 33rd anniversary of the Americans with Disabilities Act (ADA) being signed into law and so has become Disability Pride Month. Most people started today unaware of either of these events and have likely never seen the Disability Pride Flag before. You won’t likely see companies changing their logo on social media to celebrate their disabled employees and customers. Disability awareness campaigns and sharing “inspirational” disability stories may be a common part of public discourse, but Disability Pride and the history of Disability culture are less commonly discussed.
The ADA was an important milestone for the rights of people with disabilities. However, disability rights in the US have a much longer history than just the ADA and I encourage everyone reading this to take the time to learn about the larger Disability Rights Movement through resources like the movie CripCamp, the books listed at the end of this post, and by learning about specific events such as the Capitol Crawl or the Mad Pride Parade. The ADA is a moment in Disability history; it was not the end-all solution and disability discrimination and segregation still exists.
Why do I care about this topic?
Because 1 in 4 of American adults have a disability, making up over 13% of the general population, and it is the only demographic that we all will fall under at some point in our lives.
Because countless barriers have led to an immense health disparity where 1 in 3 adults with a disability do not have a usual healthcare provider and 1 in 3 have unmet health care needs due to the cost of that care.
Because I am a genetic counselor with a genetic disability. I identify as Disabled and work in a profession (genetics) with an entangled history and relationship with eugenics.
As a genetic counselor (GC), I believe that we GCs are in a unique position to dismantle barriers disabled individuals face and to move healthcare away from the historical medicalized approach to disabilities, which views disabilities as a problem to solve or something to pity. Disability Pride Month is important because disability can be more than a diagnosis, it can be a community, a legacy, and a culture with our own art forms and language use. We have these ingrained assumptions that to be disabled is to be unhappy or isolated. But I am capital-D Disabled because this is my identity; one that brings me joy and connects me to a larger movement. Disabled is not a bad word. It is important to remember this, and to remember that disability conversations are not just relevant to patient care, but also how we interact with our coworkers and students.
“Disabled people have always existed, whether the word disability is used or not. To me, disability is not a monolith, nor is it a clear-cut binary of disabled and nondisabled… Disability is pain, struggle, brilliance, abundance, and joy. Disability is sociopolitical, cultural, and biological. Being visible and claiming a disabled identity brings risks as much as it brings pride.”
― Alice Wong
In graduate training I was taught about diagnoses from the medical perspective, i.e., defining a condition by its list of symptoms, and this does have an important role in medical training. However, only teaching the medical and social model or with case examples of disability culture (i.e., the Autistic and Deaf communities) gives the false impression that various models of disability are optional lenses to try on or a “special-interest” topic. When we view a positive test result as bad news, we’re defaulting to the tragedy model of disability. When we refer patients to diagnosis-focused foundations or organizations run by parents, we are often ensuring that the charity and inspirational models of disability are the first a patient encounters because that framing of disability is best for fundraising. When we frame a condition or disability as something to fight against (i.e., the epidemic of autism), we are framing someone’s very existence as something to be defeated. We can do better than this.
I truly believe that the best way to improve how we counsel patients is to improve how we think about disability. Word choice is incredibly important, but just changing how we speak or write, while not changing how we think, means that we will continue to perpetuate outdated and detrimental ideas of disabilities as a problem to be solved. There are some easy changes in word choice we can all apply (see table at the end), but the harder part is checking our own privilege and realizing that we will spend our entire lives unrooting our ingrained biases.
Here are some quick gut-checks for ableist biases:
Have you ever seen a diagnosis on a patient chart, or a long list of them, and thought that this patient would likely be “crazy,” difficult, or a hassle?
Has your first thought upon seeing a positive test result been about the burden this is going to place on the family or have you started a disclosure with “I’m sorry?”
Have you shared “inspiring” videos of disabled people completing normal activities such as playing a sport, graduating school, getting married, or the videos of a kid using a hearing aid for the first time?
Have you told someone with a disability that you “get it” because you did a training about their condition, you once had to use a mobility aid after an injury, or you know someone with a similar condition?
When a patient doesn’t fit the textbook definition of a condition or does not provide an organized/linear medical or family history – have you considered that they are making it up or shouldn’t be believed due to being a “poor historian?”
Have you made the assumption that all disabled individuals would want a cure, treatment, or therapy (such as those designed to teach disabled people to mask their symptoms)?
Do you use disability slurs like stupid, lame, dumb, idiot, blind, deaf, crazy, or insane, such as in reference to a politician you dislike?
As GCs, we can get caught up in excitement over the latest “cool” genetic testing technology available to patients. But, I don’t think we often take the time to pause and think about the implications of what we’re offering and the assumptions these offers make. With ASRM recommending health conditions that should disqualify oocyte donors, are they sending a message of who is “worthy” of procreating or implying that their offspring wouldn’t be “optimal?” When ACMG recommends carrier screening tiers based on the “severity” of conditions, aren’t we telling Disabled people that their daily life is “impacted enough” to be a potential burden to their families and society? So many individuals who do not have disabilities and organizations decide they can speak for Disabled people and they know what is best for us. Our lives are held up as examples to justify discriminatory medical recommendations and political opinions, under the guise of “good intentions” they hijack the rhetoric of the disabilities right movement. If our voices aren’t included, and if we’re used as examples of reasons why more of us should be prevented from existing, you’re not promoting equity and inclusion. We often discuss disability rights only in the context of prenatal or preconception counseling, but being disabled is far more complex. It intersects with every single aspect of your life, and your relationship with it may change through every stage of your life. Within our current society, even existing in the world as someone disabled can be a radical act.
I think as a GC, we often want to make things simple and easy for our patients, but we cannot fear the complex and our patients won’t be able to avoid their own complex interactions with society. I’ve seen GCs dodge talking about mental health family history and avoid testing that may result in variants of uncertain significance – and I truly believe this often stems from a preconceived notion that uncertainty is, by default, a burden. If we can’t offer a “cure” or a yes-or-no answer we may get uncomfortable or feel like we’re failing our patients and then assume our patients will also be uncomfortable. However, as someone with a progressive genetic syndrome, my entire life is uncertainty. We all carry thousands of genetic changes and dozens of genetic conditions – and we need to normalize that for our patients. All of our lives are uncertain. We need not shield our patients from this normal part of life based on the belief that genetic uncertainty is exceptionally difficult. We have to be careful that we’re not continuing the collective fiction that genetic testing somehow guarantees a particular predicted future. Just because we have good intentions doesn’t mean our actions do not perpetuate harm.
Providers may warn patients to avoid social media; however that is also where a disability identity and second-family may be found. Providers may not want to “burden” patients with too much information, though who gets to decide what information should be included? We put patient autonomy and informed consent as a top priority, but the medical field also will often restrict the rights of disabled patients, for example from deciding to transfer an embryo with a genetic syndrome during IVF. ASRM recommendations for egg and sperm donors promote both positive and negative eugenicsthrough both private and public decisions. However, this puts an immense weight and emphasis on a test result – do they really give “yes or no” answers or holistic predictions about someone’s future? I think we all know that’s not true, and a genetic diagnosis (or lack thereof) is only one detail of a life being created. All pregnancies and futures are uncertain, that’s one of the joys of parenthood (and life) – very few things can truly be predicted. Our patients deserve the agency of making these decisions for themselves, with their priorities front and center, with information that’s not focused on easing the conversation at that moment or asking for an immediate decision. Our training makes us especially equipped to fight the patronizing approach of doctors knowing “best,” that was the norm in medicine for so long.
We are uniquely positioned to provide validation and support for our patients during the diagnostic odyssey, as we often have time to build those relationships and can be involved in the consent and disclosure process for genetic testing. To maintain our ability to support patients, we need to remind everyone that there is value in time spent with patients and push back against the increased pressure to shorten that time or have patients make decisions based on one-session with a GC. We need to continue to fight for unbiased GCs and to recognize that no decision is made in a bubble and even the best intentions of being non-directive, still exist within an ableist society. We need to remind ourselves that all patient reactions are normal – being overwhelmed, disorganized, confused, stress-free, happy, or proud. Our patients are not less validly disabled if they can work or if they’re on Social Security Disability Insurance (SSDI), if their disability is visible or invisible, if they have a known genetic etiology or not. What is notvalid is for GCs to feel we have learned “enough” about disabilities, to approach a patient starting from a position of skepticism, to feel like some disabilities are more legitimate than others, or to think that we aren’t ableist because we may feel like we are more of an ally than other health professions. We are ALL ableist, even those of us who are also Disabled.
“Navigating ableist situations is like traversing the muckiest mud pit. Ableism runs so deep in our society that most ableists don’t recognize their actions as ableist. They coat ableism in sweetness, then expect applause for their “good” deeds. Attempts to explain the ableism behind the “good deeds” get brushed aside as sensitive, angry, and ungrateful.”
― Haben Girm
One class in our training, one sponsored webinar, one panel at a national conference – none of these are one-stop-shops for retraining our brains to remove entrenched ableism. “We cannot comprehend ableism without grasping its interrelations with heteropatriarchy, white supremacy, colonialism and capitalism.” (Leah Lakshmi Piepzna-Samarasinha) Ableism is intersectional and complex and it will take a lot of time to unpack. I like the garden metaphor for our brain – we can’t always choose what concepts were planted in our minds in the past, it’s not always our fault if weeds flourished when we weren’t looking. However it is our responsibility to take the time to dig out those weeds and to nurture the plants we want to grow. Is weeding out ableism difficult? Yes. Is it sometimes embarrassing to realize what biases have grown in our minds? Yes. Will we spend our entire lives weeding? Probably. But that’s a good thing! When we recognize that we have a lot to learn, that we all are ableist, that this is a never-ending learning process, that is where we find our power to change and our forgiveness for our past self’s ignorance.
Advocacy is not being silent. Advocacy is having the hard conversations. Advocacy is speaking up about topics that don’t directly affect you in order to take the burden of creating change from those who are directly affected by a policy, institution, or bias. Advocacy is active. Advocacy is continual. Advocacy is humble self-reflection and strives for change.
Related Reading – contains only books I have read, so is not a comprehensive list:
Demystifying Disability: What to know, What to Say, and How to be an Ally by Emily Ladau – A quick easy read
Disability Visibility: First-Person Stories from the Twenty-first Century by Alice Wong
Care Work: Dreaming Disability Justice by Leah Lakshmi Piepzna-Samarashinha
Being Heumann: An Unrepentant Memoir of a Disability Rights Activist by Judith Heumann
About Us: Essays from the Disability Series of the New York Times by Jonathan Todd Ross
The Boys in the Bunhouse: Servitude and Salvation in the Heartland by Dan Barry
Imbeciles: The Supreme Court, American Eugenics, and the Sterilization of Carrier Buck by Adam Cohen
What Doesn’t Kill You: A Life with Chronic Illness – Lessons from a Body in Revolt by Tessa Miller
Haben: The Deafblind Woman Who Conquered Harvard Law by Haben Girma
Ask Me About My Uterus: A Quest to Make Doctors Believe in Women’s Pain by Abby Normal
Disfigured: on Fairy Tales, Disability, and Making Space by Amanda Leduc
The Future is Disabled: Prophecies, Love Notes, and Mourning Songs by Leah Lakshi Piepzna-Samarashinha
Feminist Queer Crip by Alison Kafer
We’re Not Broken: Changing the Autism Conversation, by Eric Garcia
GC and Disability related reading (may contain outdated terms and references):
Choosing Children: Genes, Disability, and Design by Jonathan Glover
Genetic Dilemmas: Reproductive Technology, Parental Choices, and Children’s Futures by Dena Davis
Babies by Design: The Ethics of Genetic Choice by Ronald Green
Telling Genes: The Story of Genetic Counseling in America by Alexandra Minna Stern
Fables and Futures: Biotechnology, Disability, and the Stories We Tell Ourselves by George Estreich *Recommended by other GSF GCs
Disabled, has an IEP/504 plan, receives additional supports in *** subject areas, support needs **
Disability/handicapped bathroom/parking
Accessible bathroom/parking
Wheelchair bound/confined
Wheelchair user, uses mobility aids *list them out
*Many of these are context dependent and so it may be okay to use certain words in certain contexts, some may also be reclaimed or the preferred term by individuals.
Devin Shuman (she/her) is a genetic counselor at Genetic Support Foundation who has mitochondrial DNA depletion syndrome. On twitter at @DevinShuman.
Beatrice Adler-Bolton and Artie Vierkant’s debut book Health Communism makes a remarkable case for reimagining the global healthcare landscape. For the genetic counseling field, their case offers an urgently needed approach to patient advocacy.
In 1995, Dr. Judith Melki isolated SMN1, a gene implicated in the rare neurodegenerative condition spinal muscular atrophy (SMA). Dr. Melki also discovered SMN2, an unexpressed near-identical copy of the SMN1 gene that was a promising target for novel therapeutics.Spinraza, the first developed from this discovery, was the product of a collaborative effort financed by orphan drug policies for rare diseases. Consequently, Spinraza was expensive, initially priced at $750,000 for the first year of treatment and $375,000 for subsequent years. The economics of Spinraza’s distribution resulted in slow uptake in both private and universal payer systems, including severalnationalrestrictions and one outright denial in its coverage on cost-benefit-grounds. In the interim, two more therapeutics for SMA had been approved: a one-dose gene therapy marketed as Zolgensma that is the single most expensive-per-dose pharmaceutical in the world at $2,125,000, and an oral maintenance medication marketed as Evrysdi that is priced on patient weight with a maximum cost of $340,000 per year.
The economic barrier to treatment for patients with SMA speaks to both the wasted utility of pharmacology in personalized medicine and what Beatrice Adler-Bolton and Artie Vierkant call the “vulgar phenomenon” of health in their debut book Health Communism. They argue that how health is defined under capitalism has as much to do with obscuring the architecture of economic systems that underpin it as it does explaining physiological phenomena. In the case of therapeutics for SMA, “personalized” also incorporates an individual’s economic, political, and geographical conditions; in other words, medicine is personalized to a patient’s class, too.
The authors explain how our global healthcare landscape was made this way with an analysis of the relationship between the many intersecting threads of medicine and economics. Their analysis coalesces arounda theory of healthcare delivery called Extractive Abandonment that functions primarily as financial extraction of the working class and global south. An intersection of Marta Russell’s “money model of disability” and Ruth Wilson Gilmore’s theory of “organized abandonment” in the US prison system, materially Extractive Abandonment simply concentrates wealth among the ruling class. However, sociologically it fuels the production of narratives around the worker/surplus binary – an iteration of the “eugenic debt burden” of the twentieth century – which aim to naturalize it in our culture. In an American context, it is no coincidence that healthcare’s ties to employment are the product of labor bargaining. In the authors’ words:
“The worker/surplus binary solidifies the idea that our lives under capitalism revolve around our work. Our selves, our worthiness, our entire being and right to live revolve around making our labor power available to the ruling class. The political economy demands that we maintain our health to make our labor power fully available, lest we be marked and doomed as surplus. The surplus is then turned into raw fuel to extract profits, through rehabilitation, medicalization, and the financialization of health. This has not only justified organized state abandonment and enforced the poverty of the poor, sick, elderly, working class, and disabled; it has tied the fundamental idea of the safety and survival of humanity to exploitation.”
There is not a single better explanation as to why three SMA therapeutics can be put on the market for preposterous prices, let alone put on the market at all. To put it simply, the authors quote disability scholar Liat Ben-Moshe: “surplus populations are spun into gold.”
But it does not have to be this way. Adler-Bolton and Vierkant show throughout Health Communism that the extractive economic systems that finance modern healthcare delivery are sociologically obscured but not invisible. With some work – which the authors have graciously started for us – it is possible to reveal these systems for what they are. Only then can they be changed.
Revealing one of these systems in particular, US’ Social Security Disability Insurance (SSDI), offers the genetic counseling field an urgently needed approach to patient advocacy. Adler-Bolton and Vierkant describe SSDI as a biocertification regime in which disabled bodies are not “certified” for care, but rather “de-certified” for work. In order to qualify for SSDI, a person’s disability is quantified in monetary terms with respect to a certifiable labor-limiting diagnosis. Known colloquially as “The Blue Book,” the Social Security Administration’s (SSA) medical guide for disability evaluation is the actuarial document that facilitates this biocertification, and much like the social determinants of health, it has been naturalized when it is anything but.
If the pharmaceutical industry’s drug pricing is the “extractive,” this biocertification regime is the “abandonment.” A decades long neoconservative political project has gutted the American welfare state, and another decades long neoliberal political project has plagued policy with the adverse logics of cost-benefit-analysis. What is left is a disaster worsened across the political spectrum, a fact that is the basis of critical disability studies but largely absent in today’s political imaginary.
The authors offer an important caveat about this biocertification regime, however, one that brings to mind the role genetic counselors play in the diagnosis of genetic disease: “Resisting biocertification does not mean resisting “diagnosis” or identification. It means resisting the leveraging of these certifications by capital and the state.”
Those impacted by SMA, for example, are forced to pay astronomical costs or navigate administrative burden whether they are certified for treatment through economic means or their bodies de-certified for work by the state. In either circumstance a genetic test is going to be involved, one that may even incur its own monetary cost.
It is worth noting that these genetic testing options, much like the SMA pharmaceuticals discussed earlier, are miraculous. The ability to accurately identify genetic disease is an invaluable resource and as Adler-Bolton and Vierkant say it should not be resisted. However, genetic testing plays a straightforward role as a prerequisite for therapeutics or care, and is as such complicit in reinforcing the monetary valuation of life.
This says nothing of the quality care provided by the genetic counselor who facilitates the discussion around the ordering of the genetic test, the precision of the biotechnology and bioinformatics that perform it, nor the careful review of the analysts who classify a result. These are integral aspects of our healthcare infrastructure. What it speaks to is how the process is leveraged by the pharmaceutical companies described earlier, and by the state. When aspects of health inequity are described as being “institutionalized,” this is what is meant.
As genetic counselors, we’re often a first touch point for individuals affected by genetic disease, and facilitate triaging to other medical specialties and care resources. What Adler-Bolton and Vierkant make clear in Health Communism is that the priorities of the systems and institutions in this triaging process are extractive in nature. So if our aim as clinicians is to improve the quality of life experienced by individuals affected by genetic disease, then we must first acknowledge these systems for what they are.
While the monetary extraction by the pharmaceutical industry is blatantly obvious, the abandonment by the state is more subtle, and is marked by indifference. It involves significant administrative burden to provide poverty-wage benefits. To explain, let’s look at the SSDI determination for individuals affected by SMA. While according to Social Security Ruling (SSR) 16-4p: Titles II and XVI, “With the sole exception of non-mosaic Down syndrome, genetic test results alone are not sufficient to make a disability determination or decision,” they are central to the determination process. For example, the “Suggested Medical Evidence of Record (MER) for Evaluation” policy for disability determination of someone with SMA is molecular genetic testing of SMA1, a misspelling of the SMN1 gene. It is both baffling to think this misspelling persists through document reviews and infuriating to consider whether it has led to an SMA patient’s SSDI from ever being denied and further administrative burden.
This is the true face of the system genetic counselors can provide to people who are suffering. It is an embarrassment. There is not a single better explanation as to why an SSA document could have such an egregious error than what Adler-Bolton and Vierkant present in Health Communism.
What does this mean? It means as genetic counselors we have work to do, work we were already scheduled for. The Accreditation Counsel for Genetic Counseling (ACGC)’s nineteenth practiced based competency asks that genetic counselors advocate for individuals, families, communities, and the genetic counseling profession. The twenty second practice-based competency asks that genetic counselors recognize their role in the larger healthcare system.
Our field has a serious problem, and it is about time we recognize it. One way we can start is by asking hard questions. Here is one that I have: How does an emphasis on patient choice regarding testing – an aspect of the genetic counseling delivery model built around the medical ethical principle of autonomy to create distance from a eugenic past – reinforce the logic of healthcare as a commodity to be sold in the private market?
Dan Meadows is a genetic counselor and competitive cyclist based out of Fort Collins, Colorado. He can be reached at danmeadows@pm.me
by Kimberly Zayhowski, Helen Kim, and Liann Jimmons
As we are reminded by the National Society of Genetic Counselors’Professional Status Survey each year, the genetic counseling field remains notoriously homogenous. With the Black Lives Matter and Stop Asian Hate movements and a growing consciousness of social justice matters, many with privileged identities are coming to appreciate the extent of oppression such as racism, sexism, ableism, transphobia and homophobia in our society. A focus on diversity, equity, inclusion, and justice (DEIJ) has been highlighted inNSGC’s initiatives in recent years. This surge in DEIJ work gives us optimism. At the same time, it’s important that allies are diligent at monitoring their own motivations to not become opportunistic “allies” who capitalize on DEIJ work to bolster their social capital and CVs. In many spaces, false allies are proceeding with DEIJ work as a grant-funded trend while actually harming the communities they are supposed to be serving. When people focus their effort into having others view them as “allies,” they may obscure their complicity. In this piece, we outline some of these problems and offer an opportunity for constructive reflection so that we can all work towards something genuine.
Nascent in their journeys in DEIJ, there are a number of ways well-meaning allies contribute to the erasure of community members. DEIJ work can be another way white, non-disabled, straight, and/or cisgender folks colonize marginalized spaces.Columbusing behavior, or “discovering” something that is not new, is a symptom of internalized white supremacy. Even if someone has “found” new knowledge about a marginalized community, that fascination can easily turn into fetishization. Without the context and rigor of lived experience, the understanding of these social dynamics can only remain superficial. Work that lingers at contemplation, theorization for the sake of it, and reiteration of known problems without real solutions remains ineffective. With this, non-community members become viewed as “experts” and hold authority on topics on which they only have an academic understanding. It leads to the hoarding of diversity-related positions or projects and gaining visibility, recognition, and financial compensation for said work. Academic work without community involvement or benefit becomes a means to an end, another way of objectifying minoritized people’s struggles. Internalized white supremacy is insidious in nature and requires constant checks and balances. Power is being siphoned away from minoritized scholars in their own communities as opportunities are lost to outsiders who have better connections and systemic privilege.
Communities need respect and dignity, not “allies” who profit off of their oppression. While non-community members may be well-meaning and spurred by their new understanding of racism, transphobia, ableism, and/or homophobia, pursuing work in these areas without the leadershipof marginalized community members can become disingenuous and opportunistic. For example,one survey found that ~76% of chief diversity officers are white, while ~4% are Black, ~8% are Latino or Hispanic, and ~8% are Asian. Organizations continue to hire workers who have little or no experience to execute DEIJ missions. Putting non-community members in positions of power related to diversity work is underhanded and waters down what work can actually be done. Without community engagement, even the most well-intended non-community member will miss key information and insight that is pertinent to drive change.
Proximity does not equal identity. Authorship does not equal embodiment. It is imperative that allies who are working in DEIJ spaces cite, partner with, and support scholars from minoritized communities to take the lead on DEIJ initiatives. It is both true that allies can do meaningful DEIJ work AND that we need to be critical when leaders in these spaces are promoting themselves as experts on identities and experiences that are not theirs.
The difference between supporting and exploiting
The people who receive the most publicity are often those with the loudest voices, but they are not always the necessary voices. It can be easy to make the excuse that you cannot find a community member to lead an effort. However, if you are truly invested in making a difference and supporting historically marginalized communities, you need to put more effort into finding a voice to amplify louder than your own. People with privileged identities need to step up in ways that uplift not overtake. It is true that allies have opened doors in meaningful, necessary ways, but it’s imperative that we all recognize when to transfer the power back. Open the door and hold it open for someone else to walk through.
So where is the line? How do we recruit without tokenizing, how do we include without exploiting, and how do we take action without colonizing opportunities? Some critical questions for allies who aim to empower (not overpower) minoritized communities to consider when engaging with DEIJ work:
Presentations: Are you the right person to give this presentation? Do you know of a community member you can recommend for the presentation instead? Can you advocate for pay for DEIJ-related presentations? If you take on a presentation, should you bring in a co-presenter? Are you in a position where you could mentor someone with needed perspectives who has less presentation experience?
Research:How do you position yourself in relation to the research question? How do your identities impact decisions made throughout the project? Are the goals of the project in line with community-expressed needs? Do you have diversity on your team, including folks with lived experiences relevant to the project? Are your community consultants worthy of authorships instead of acknowledgments?
Leadership roles: Are you the best person for this position? Is your perspective already represented in this space? Is the selection process inclusive? Can you use your privilege to elevate another candidate instead and support the project or institution in an alternate way?
Overall:Take some time to understand all of your incentives and motivations behind doing this work. Share them with friends, colleagues, and mentors you trust to tell you when you’re in the wrong. Find opportunities to be vulnerable and solicit feedback. Spend a lot of time in this phase of your work before jumping in recklessly. Be in community with folks able to give you iterative feedback and commit to this process. Are there other perspectives you should be bringing in? Is your work transactional? What are your intentions? Are you only involved in anti-oppression work that results in additions to your CV? Do your intentions align with the impact? Is your work being done to drive change or just to make you feel better about yourself?
All in all, while allies must do the legwork on tackling DEIJ issues, we emphasize leg. While minoritized folks should lead changes that affect their communities, they cannot continue to shoulder the entire weight of this work by themselves. Whenever possible, community members must be at the head of the efforts, and allies need to examine how they can redistribute their power. We highlight the needs for collaboration with community members and accountability at all levels to ensure that our actions and impact are in line with our intentions. As individuals, institutions, and systems, we need to scrutinize the impact of our actions on communities, develop our awareness to see beyond ourselves, and dedicate ourselves to doing better.
Note: This is a call to engage in honest self-reflection about our motivations as individuals, not a call to persecute our colleagues. We feel strongly that people should not have to publicly disclose personal aspects of their identities while doing DEIJ-related work. We also recognize many identities are fluid and can change over time. Engaging in DEIJ work requires us to honor the trust that our colleagues give to us.
Authors
Kimberly Zayhowski, MS, CGC (she/her) works as an assistant professor and research genetic counselor in Boston, MA. Her views are informed by her queer and multiracial identities.
Helen Kim, MA, MS, CGC (she/her) is a chronically ill and queer genetic counselor. She is an educator and public engagement associate working to foster conversations around ethical and societal implications of genetic technologies with minoritized communities in Los Angeles, CA.
Liann Jimmons, MS, CGC (she/they) is a genetic counselor and, more importantly, an advocate for genomic justice. She works in public health doing outreach, education, and clinical services for underserved communities in Honolulu, HI.
Polygenic scores (PGS), sometimes referred to as polygenic risk scores (PRS), are a developing risk estimate tool used to determine personalized risk for complex conditions that are influenced by both genetics and environment, such as breast cancer. Historically, utilization of PGS in genetic testing has been discriminatory and inequitable across various ancestries, which likely exacerbates racial inequities. While genetic ancestry is biologically based, it can correlate with race (a social construct); therefore, inequities in ancestry-based data add to racial health care disparities. Until 2021, PGS for breast cancer was only available to cisgender women of self-reported European ancestry due to a lack of sufficient GWAS data to identify relevant SNPs among other populations. Events of 2020, including the murder of George Floyd, sparked the country’s short-term widespread awareness of, and engagement in, addressing racial inequality. The country’s reaction, combined with increasing pressure from many individuals in the genetics field concerning the racial inequality of PGS, resulted in some changes in reporting practices of PGS. Laboratories who previously offered this testing updated their test menus; some removed PGS testing, while other laboratories released updated versions.
Despite modifications, it has been demonstrated that PGS are still not equitable across ancestries. As genetics providers, we require transparency in marketing materials, equal discriminatory power across all populations, and demonstration by genetic testing laboratories of true commitment to reduction of healthcare disparities before use of PGS can be considered equitable and able to be used across ancestries.
In November of 2022, Hughes et al. published an updated PGS for breast cancer they call “multiple-ancestry polygenic risk score” or “MA-PRS”. The authors developed a breast cancer risk assessment with greater accuracy for cisgender women of non-European ancestry by adjusting the weight given to each single nucleotide polymorphism (SNP). This MA-PRS uses 56 ancestry-informative SNP markers to determine the patient’s proportion of African, East Asian, and European ancestry. It then weighs the 92 previously identified breast cancer-associated SNPs based on the relative proportion of each ancestry.
The National Society of Genetic Counselors (NSGC) and Wand et al. have recently published a Practice Resource on PGS which argues that “equitable access to polygenic scores is threatened by differential test performance across populations, differential capacities to support population-wide delivery of genetic services, and differential resources for [PGS] education or uptake of information in a population.” Similarly, there is a new statement on clinical application of PGS published by The American College of Medical Genetics and Genomics (ACMG) and Abu-El-Haija et al., which includes the need to “improve available data sets for populations with non-European ancestry and optimize analytic methods [of PGS] so that genomic risk can be accurately and equitably identified across all human populations.” While the MA-PRS attempts to ameliorate some of these disparities, we argue that significant barriers to equal access remain.
In addition to these concerns regarding equity and access barriers related to the MA-PRS, there remains a significant question regarding the clinical utility of PGS. Currently, the National Comprehensive Cancer Network (NCCN) guidelines expressly counsel against using PGS results for clinical decision-making due to a lack of proven clinical validity. Therefore, insurance coverage for any medical management based on an elevated PGS score is highly in question. Similarly, the NSGC Practice Resource states, “clinical utility of [PGS] remains largely hypothetical, with increasing research evaluating clinical outcomes.” Furthermore, “genetic counseling about [PGS] should be framed in the broader context….[PGS] often does not capture all genetic risk.”
Considering the remaining disparity in clinical validity among populations, the complexity of PGS results interpretation, the lack of demonstrated clinical utility, and the potential lack of insurance coverage, we argue that significant work from the genetics community is still needed in order for PGS to truly be equitable and clinically useful. We acknowledge that MA-PRS are a first step towards that goal, but additional improvements need to continue.
As laboratories continue to improve or develop PGS, we ask for the following:
Transparency by genetic testing laboratories offering PGS.
Is this PGS performing equitably across ancestries? If marketed towards diverse patient use but without actual equal performance this could be misleading at best, and potentially harmful to patients at worst.
Is there clinical utility currently for this PGS? Providers should not be told that PGS will help with clinical management and qualifying for high-risk cancer screenings so long as NCCN and other governing bodies recommend against such.
Validation and equal power across all populations.
Who can use this PGS? Given the development of PGS for use in non-European populations, there should not be movement backward. All future PGS options should be available and validated in diverse populations.
How well does this PGS perform in diverse populations? There should be equal power and validation across all ancestral groups; it should not perform better or worse for one group over another.
Demonstration of true commitment to inclusion and equity for patients by addressing underlying barriers.
What research and data is this PGS based on?Eighty-four percent of GWAS participants in cancer risk studies are of European ancestry. This GWAS data has been the foundation of all genetic testing (including PGS). We encourage researchers to foster a culture of transparency and trust with underrepresented populations with goals of obtaining ancestrally diverse representative data. Therefore, allowing for development of wholly new PGS and mitigating the need to reanalyze the currently available and ancestrally limited data.
What relationships are involved? Who are the collaborators? Bias exists in many areas of medicine; limiting that bias should be done whenever possible. Collaboration with and funding for groups specifically focused on diverse experiences, such as patient advisory boards and community-based participatory research projects, should be prioritized.
How are other barriers or health disparities being addressed by laboratories offering PGS? Health disparities in genetics, such as access to genetic counselors or germline testing and higher rates of variants of uncertain significance for patients who are from underrepresented populations, already exist. As mentioned, although race is a social construct, disparities of testing and healthcare based on ancestry further exacerbate racial inequities. True commitment to inclusion and equity does not stop at PGS. Rather, it is necessary to address across all areas of genetics and throughout other health care specialties.
If you agree, join us and please sign this petition to register your support for transparency, validation across populations, and true commitment to inclusion and equity from PGS producing laboratories. These are the opinions of the individuals listed below, and not their institutions.
My professional life up till this point has been centered around a mission to bring genetic counseling to people who – like me – live with psychiatric conditions, and their families. This has been my mission for >20 years, since my family started asking me about whether psychiatric conditions were genetic and what this meant for us while I was doing my PhD on this topic. Realizing that it wasn’t just my family that had these questions and that no-one was really addressing them is what drove me to train as a genetic counselor. Once I completed my genetic counseling training in 2003, no one would hire me to provide genetic counseling for families with psychiatric conditions. Of course, psychiatric conditions have always been profoundly disenfranchised in terms of health services, but as well, there was no evidence that people with psychiatric conditions wanted genetic counseling, and no evidence that it could help. So, this drove me into research.
I landed a research professorship and my team and I generated data showing that:
people with psychiatric conditions wanted access to genetic counseling
genetic counseling helps people with psychiatric conditions
In 2012, on the strength of these data, we established the Adapt clinic – the world’s first specialist psychiatric genetic counseling clinic. It was all about helping people understand the factors that contribute to developing a psychiatric condition, and how to use this understanding to engage in self-management strategies to protect their mental health for the future. It was about helping people to make meaning, and understand that psychiatric illness is not your fault, and not your fate.
In 2023, after 11 years of helping patients, training students, generating research data about the impact of what we do, and providing a model for psychiatric genetic counseling services around the world, our service is being closed.
I’ve fought this with everything I have because it feels so wrong. But I’m so bone tired …and there’s literally nothing more I can do. It’s over.
No amount of data demonstrating the awesome outcomes that patients experience (increases in empowerment, changes in behavior to engage in self-management strategies to protect their mental health) after receiving our services has swayed the decision. So, this is a eulogy.
The webpage for the clinic has silently ceased to exist.
The reason given for the death of the Adapt clinic? To redeploy the counselors to provide service for general genetics patients because the waitlist there is so long. It’s apparently that simple. And pointing out that this is classic disenfranchisement of people with psychiatric conditions – again, people like me – has made no impact. I may as well be speaking to a wall.
Now, as someone who has served as a leader myself in a publicly funded healthcare setting, I do of course understand that we are forced to make decisions about how to allocate scant resources. And sometimes people might not like the choices we make. I understand that. My objection is that the Adapt clinic embodies (has embodied) all of the principles and values claimed to be held dear by the healthcare system that is closing it. That is what I find distressing.
Initially, when I saw the writing on the wall that the clinic would be closed, I was devastated- this was my life’s work, I thought. And it’s been for nothing, my internal voice said…I am a failure. I lost all energy to continue in my efforts to leave things better in the world than I had found them. Because, what is the point? I – and the counselors within it – gave the Adapt clinic everything we had, it was demonstrably successful, and yet it is still being closed….it felt like it was all for nothing.
But this narrative is wrong. I can see that I am not a failure, and that the clinic was not a failure. Instead, the clinic, and the counselors within it, and the patients we serve, have all been failed by the system we are in.
Our efforts were not for nothing. The Adapt clinic has helped about 1400 patients and trained over 50 students, some focused on clinical skills, some focused on research skills, and some both. We published about 20 papers that are out there in the world that explain the difference that psychiatric genetic counseling can make for people, and how to do it well. I know that we have inspired practicing genetic counselors around the world as well as students…we have inspired people to train in this discipline. I know this because people have been gracious enough to tell me about how our work has affected them.
Given all this, you have to ask, why is the clinic dead? I think there are two real answers to that. First, psychiatric conditions are still so stigmatized. People with mental illness – like me – have a long and awful history of being disenfranchised, and here we see it again: an evidence-based service for people with psychiatric conditions cut, despite data showing that it’s needed and it helps. And yet it’s cut so that we can prioritize providing services for people with non-psychiatric indications.
Second, the genetic counseling services we provide for people with psychiatric conditions typically don’t involve genetic testing. And though the service helps people, the health system decision-makers don’t value genetic counseling when there’s no genetic testing being done. The psychotherapeutic work we do is not valued …which is truly the hardest thing for me to swallow, because data show that it’s exactly this that makes the difference even when genetic testing *is* available. It’s the counseling that helps people.
So, yes, this is a eulogy — a public expression of pain and grief and disillusionment about the death of a clinic whose establishment was the culmination of >10 years of my work, that we nurtured successfully for 11 years, and that brought purpose to my life and a way to channel my own experience of psychiatric illness to help others. It’s so hard to build and create something new and innovative, and so very easy to destroy it. It does feel like a death.
My biggest fear is that others will stop trying to establish psychiatric genetic counseling clinics in other jurisdictions as a result of this. People – like me- who have psychiatric conditions deserve better than this. So please keep pushing. Others have taken up the mantle – there’s a clinic in Cardiff, and Tennessee, and others (if you know of others, please tell me!)… I’m rooting for all of you. Please let me know how I can help.
But I think this reflects broader issues too – I think as a profession, we have to answer some questions for ourselves. Are we happy with being reduced to roles as the purveyors of genetic testing? And only post-test counseling at that? This is the direction in which we are headed. Medical genetics departments with long and growing waitlists often respond by simply reducing the list of indications to make fewer people eligible to access genetics services. That’s exactly what happened to the Adapt clinic — the eligibility criteria for access to genetics services shrank to exclude our patients. What happens to these patients? It’s not that they get service elsewhere – they don’t. The people who make these decisions are deciding who gets care — deciding who matters. This is an issue that relates to equity and justice.
In writing this eulogy for the clinic that I created and loved, my purpose is to try to use its death for something positive. Given our increasing focus on the importance of EDI issues, I would like to suggest that this is an opportunity to question whether tertiary-care clinical genetics is the right location for genetic counselors if we are to be able to provide just and equitable access to our services for people who need them. Situating genetic counseling services in alternative locations, such as primary care/family practice, might be worth considering as a way to ensure our ability to practice to the top of our scope, to offer more than just genetic testing (like psychiatric genetic counseling), and to ensure more equitable access for patients.
I hope that the end of Adapt can be used as an impetus for the start of something new. If the Adapt clinic has impacted you in some way, those of us who nurtured it would love to hear about it in the replies, or by message.
Some of my fave quotes from people who had psychiatric genetic counseling in the Adapt clinic (from Semaka et al 2019):
“Until genetic counseling, no one ever coherently explained to me why I have a mental illness. And I think that’s a conversation that needs to be had because most people just think they’re having a bad time of it or they just think that they just need to try harder”
“I felt in control, you know [psychiatric genetic counseling] made me feel more empowered than I did when I walked in and I think for me that’s a big deal… I just felt after the appointment I had more tools to control my life.”
“[Psychiatric genetic counseling] gets rid of some of the shame…. with mental illness, it’s so hard to know what you did wrong but really you didn’t do anything wrong and [psychiatric genetic counseling] just explains that to you… so you’re able to look at this and think, ‘OK, this isn’t my fault’”.
Pedigrees have long been the backbone of genetics. Not surprisingly, therefore, we tend to think of pedigrees as primarily medical tools for analyzing inheritance patterns, assessing risk, and conducting research, as well an opportunity to elucidate the dynamics of family relationships. But pedigrees and the various other graphic, textual, and oral descriptions of family histories have played many roles over time and across cultures. These familial maps provide insight into the underlying and sometimes nefarious motives and goals of the mapmakers.
Here I propose 14 additional reasons family histories might be recorded, beyond clinical genetics. There is some overlap in these categories; the world has a tendency to not fit into neat and discrete categories. The Good Readers of The DNA Exchange might think of additional functions, and I encourage you to add your thoughts in the Comments section.
1. Curiosity About ”Blood Family”: Who were my ancestors? What were their lives like? How do they and their lives affect my life? Oral traditions of genealogy probably go back to the dawn of humanity. Starting around 4 centuries ago, as reading, writing, and education became more commonplace, the practice of recording a family history in graphic or text form started to become more commonplace. Think of the now largely forgotten tradition of The Family Bible, with its record of births. Or of folk art family trees with images of ancestors hanging from its branches. The widespread availability of relatively inexpensive DNA ancestry testing and online genealogical tools, along with genealogy-based TV shows like Finding Your Roots, has led to an explosion of interest in exploring and recording family histories. Of course, some people find out that “blood family” isn’t exactly who they thought it would be, which can disrupt familial relationships and lead to a whole host of complicated issues.
A mid-19th century American Family Tree, family name unknown (photo taken by the author at the American Museum of Folk Art in New York City).
2. Political: Pedigrees have long been tied to establishing the hereditary legitimacy of royalty to rule over a people. Some scholars argue that the words king and kin are etymologically related, and the oldest etymological sense of the word queen seems to simply be “wife.” European genealogies, especially among Germanic peoples, were described prior to the 11th century but these were mostly succession lists of kings (often, but not always, father to first-born son) or attempts to trace ethnic origins to a mythological ancestor. One of the earliest surviving royal pedigrees is of the Carolingian Dynasty, created in the early 11th century, some 200 years after the death of Charlemagne. In various versions of this pedigree, relatives were added or subtracted to legitimize claims to rule some of the lands that emerged after the empire’s collapse.
Another example of a pedigree strategically including or omitting different people, and perhaps fictionalizing some relationships, can be found in John Hardyng’s 15th century rhyming verse Chronicle. Hardying (also spelled Harding) crafted a genealogy for Richard Duke of York and his descendants that managed to legitimize the entitlement of the House of York to the thrones of Britain, France, Portugal, and Spain. Oh, and Jerusalem too, for good measure. Hardying’s chronicle also attempted to de-legitimize earlier genealogical claims to the throne made by John of Gaunt, founder of the House of Lancaster. Hardyng’s Chronicle was propaganda that served as justification for The War of the Roses between these rival branches of the House of Plantagenet.
3. Religious: Genealogies have been used to establish divine lineages for religions. The so-called Tree of Jesse, which traces the ancestry of Jesus back to Jesse, the father of David, is a classic example of this, as are the Biblical Begats that trace the lineage of Adam to Noah. By the same token, Islamic genealogy traces the Prophet Muhammad back to Abraham and Adam.
Medieval monastic orders, particularly the Franciscans and Dominicans, created monastic “family trees” (called Ordensstammbäume) with a founder at its root and various prominent members of the order branching off the tree, evoking the sense of the monastic community as a kind of family.
Some rulers traced their ancestry back to gods to legitimize their right to rule – Caesar Augustus claimed to be descended from Venus, Mars, Jupiter and Juno; the Pharaohs claimed to be descended from Ra, the God of the Sun, Sky, and other domains. The 13th century Secret History of the Mongols, based on earlier oral and written works, detailed the partially mythological ancestry of Genghis Khan. Tibetan Buddhism incorporates spiritual genealogy into its practice, based on lineages of teachers and their pupils, their pupils’ pupils, and so on. Tibetan Buddhism also uses reincarnation lineages (who gets reborn as whom) to determine religious leaders and, ultimately, the Dalai Lama as a political and religious leader.
An Abbot and His Lineage , Western Tibet, 14th Century (Los Angeles Museum County ofArt LACMA M.80.188.jpg in the public domain)
4. Legal: One of the oldest reasons for formally recording a family history was to determine the appropriate inheritance of land and property. The Roman legal text Pauli Sententiae (tr., “The Opinions of Julius Paulis”)from around 300 CE states that determining who is entitled to inherited property involves drawing up stemmata (s., stemma; essentially a form of a pedigree): “The stemmata of cognate relationships are separated by a straight line into two lines, one of which represents the ascendant and one the descendant. From the ascendant are horizontal lines starting at the second degree.”
It was also within the legal system that the word “pedigree” was first coined, in Norman-English legal documents. The word “pedigree” is actually a product of the Anglo-Norman dialect of England and did not enter “mainstream” French until the 1820s.
More recently, and more controversially, forensic genealogy has used DNA from commercial ancestry testing companies to re-construct pedigrees to identify potential perpetrators of crimes.
5.Establishing The Right to Be Assigned a Specific Coat of Arms: Coats of arms evolved from the designs on the chain mail armor of medieval knights, starting around the 12th century. The right to display a specific coat-of-arms is determined by who your ancestors are, and are assigned by a central authority, such as England’s College of Arms. Applicants for a coat must register “a pedigree showing direct male line descent from an ancestor already appearing therein as entitled to arms” with the College, which then verifies the information.
6.Ontological: Genealogies help establish a framework of reality and an individual’s relationship to the world about them. These genealogies incorporate the physical and metaphysical world. Genetic relationships may be secondary or irrelevant to such genealogies. For example, the Nekgini-speaking people of Papua New Guinea live in small villages called palems. Siblings are defined as all members of the second generation that have lived in the same palem, regardless of genetic relationship. They are considered siblings because they have a shared knowledge of the land, spirits, and food particular to their palem.
Many Native American people trace their clans – and thus to some extent their families – back to creation stories that tell how the first people came into being, sometimes from the biological realm and sometimes from the physical realm. Clan names were often derived from the animal or plant from which the clan is descended
7.Anthropological Studies of Kinship: Starting in the late 19th century, and extending well into the 20th century, kinship analysis formed a core part of ethnographic studies of what were viewed as “primitive cultures” (typically in countries that had been colonized by Western Europeans). Classic studies in the tradition of Lewis Henry Morgan, W.H.R. Rivers, and E.E. Evans-Pritchard typically imposed their Western view that genetic relationships universally formed the basis of kinship, which was often at odds with how the societies they were studying viewed kinship. Indeed, anthropologists often complained of the difficulty of trying to overlay English kinship terms and relations onto native systems and terminologies. Not every culture views relationships in terms of a branching genetic tree or genetic ancestors.
As an interesting aside, in classic anthropological pedigrees males were sometimes depicted with triangles rather than the squares characteristic of genetics-based pedigrees. This may just reflect a difference of tradition, but one could speculate that it was a conscious attempt to distance anthropology from eugenics. The image below is Margaret Mead’s pedigree of the kinship relationship system of the West African Twi from 1925 (but not published until 1937), probably just before she left to start her (in)famous fieldwork in Samoa. It is one of the earliest anthropological pedigrees to use symbols to denote people. It was drawn at Columbia University where she was a graduate student studying with Franz Boas, a founding figure of anthropology and one of the most vocal critics of eugenics. So it’s not out of the question that the triangle male could conceivably be a nose-thumb at eugenics, though I am unaware of hard evidence to support this contention. Mead’s kinship pedigree, by the way, was based on information provided by Ansa, another student at Columbia University who gave his address as Kwadjowusu, via Apegusu, Gold Coast. The text around the edges indicate the name of that relationship rather than the name of that individual, e.g., nana = any grandparent (funny how some words like nana seem almost universal). Twi relationship terms can vary with whether the speaker is a man or a woman.
8.Mate Choice: Many societies impose rules on who one can or cannot marry or have sexual relations with, dependent on the relationship between the two people. Indeed, “incest taboos” exist in virtually every society, though with different criteria as to what constitutes an incestuous or inappropriate relationship (not always limited to genetic relatives). In Western Europe where, for reasons that are not entirely clear, the Catholic Church tightly regulated marriage to genetic relatives to an astounding degree of relatedness (but also regularly granted exceptions when it was politically or economically expedient). A couple, usually royal or aristocratic, who wished to be married would submit their pedigrees to the Church, which would decide whether the union was acceptable according to relationships established by an arbor consanguinitatis, a table that laid out the degree of genetic relationship between various family members.
9.Ego Gratification and Social Status: People often search their family history in hopes of finding a Genghis Khan or a Charlemagne (statistically, it’s relatively likely that everyone has a famous ancestor). Americans like to find a relative who was one of the 100 or so people who “came over on The Mayflower,” and many Aussies find a certain pride in being descended from a transported convict. Somehow it makes you feel just that much more special.
Ancestry-based social organizations can provide a sense of shared ideology and elite status – and perhaps a distorted sense of patriotism. Membership in the Daughters of the American Revolution (DAR) is available to “[a]ny woman 18 years or older who can prove lineal, bloodline descent from an ancestor who aided in achieving American independence is eligible to join the DAR. She must provide documentation for each statement of birth, marriage and death, as well as of the Revolutionary War service of her Patriot ancestor.” Likewise, membership in the United Daughters of the Confederacy and the Sons of Confederate Veterans require an ancestor who fought for The Confederacy during the American Civil War. Members see themselves as socially privileged, based on a shared ancestry, racist ideology and false narratives about slavery and the Civil War.
10. Tools of Oppression and Conformity: As I’ve written about previously in this space, pedigrees have been used to oppress people, as happened with the American (and other) Eugenics Movements. Pedigrees could be the basis of life and death in Nazi Germany, when any Jewish ancestry could have tragic consequences. Pedigree symbols have also typically forced people into one of two genders, male or female.
11.Social Organization: Genealogy can serve as a basis for organizing social structure and social interactions. In the late 7th and early 8th century, Hishām ibn al-Kalbī authored a comprehensive and massive genealogy called Jamharat al-nasab (“The Multitude of Genealogy”) that amassed ~35,000 names and included the paternal lineages of most of the Arabian peninsula.al-Kalbi’s genealogy organized the various Bedouin tribes of the area and traced them to two ancestors, Qahtan (Noah’s great-great grandson) for the southern tribes, and Adnan, a descendant of Abraham, for the northern tribes. Arab genealogy, (nasab in Arabic), served to structure social relationships – who owed allegiance to whom, who had elite status based on being a Sayyid or direct descendant of Muhammad through his daughter Fatimah (all 3 of the Prophet’s sons died young), potential marriage partners, who could be a sheikh, and in the organizing of the diwan (networks through which money and other goods were distributed). There is reason to believe that al-Kalbī may have created some fictitious relationships and down-played the importance of some tribes, perhaps for political purposes.
Interestingly, in the early Arabic Medieval period, the human body, rather than a tree, served as a metaphor for genealogical relationships, with various parts of the body representing different segments of ancestry, starting with an entire ethnic group at the top of skull and proceeding on down to the extended family at tip of the lower extremity.
12. Describing Family Dynamics: Social Work and Psychotherapy have an equivalent to a pedigree called a genogram. A genogram looks just like a genetics pedigree but uses a variety of graphic lines that connect individuals to one another to indicate their emotional relationships (e.g., Very Close, Estranged, Sexual Abuse).
Genetic Counseling has a similar but infrequently used tool called the Colored Eco-Genetic Relationship Map (CEGRM), developed by genetic counselors Regina Kenen and June Peters in 2001. According to its authors, the CEGRM “… combines information that can be derived from pedigrees, genograms, ecomaps, and social network analysis in a single, or series of, pictorial maps based on colors and shapes. The CEGRM is based on a social systems perspective, particularly emphasizing social exchange and resource theories.”
13. Poetry/Literature: There is a very old tradition of establishing the mytho-historical origins of characters in epic poems. The genealogy at the beginning of The Iliad links the lineage of the Greek Gods to humans and to the natural world. The opening verses of the Indian epic Bhagavid Gita, which describes a battle between the armies of two cousins, lay out the familial links among various warriors on both sides. In addition to its deep spiritual messages, this epic examines the internecine and senseless nature of intra-familial conflict.
Teachers, fathers, sons, grandfathers, maternal uncles, grandsons, fathers-in-law, grand-nephews, brothers-in-law, and other kinsmen are present here, staking their lives and riches. O Madhusudan, I do not wish to slay them, even if they attack me. If we kill the sons of Dhritarashtra, what satisfaction will we derive from the dominion over the three worlds, what to speak of this Earth?
– From the opening verses of the Bhadavid Gita
In more recent times, many novels structure their narrative around the stories of multiple generations of a family, like Thomas Mann’s Buddenbrooks, Gabriel García Márquez’s One Hundred Years of Solitude, and Min Jin Lee’s Pachinko, to name but a few.
14. Dehumanization By Erasing Genealogies: Just as important as the functions of the existence of a pedigree is the absence and intentional obliteration of a genealogy. Slavery, especially in the Americas, resulted in the tearing apart of families. This started in their native lands, where families were often separated when people were forced into enslavement. Then, in the lands they were forcibly transported to, parents, children, and siblings could be further torn asunder when they were sold to different plantations, often with indifference to the family structure. Enslaved people could not be taught to read or write under pain of the lash or worse, so they could not even record their genealogy to try to maintain a record of their fractured families. Enslaved people were considered legally nameless until they were sold and some slave owners freely named their human property. Government censuses and wills often did not even give the dignity of recording names, or even just first names, of enslaved people.
The absence of a name along with eradicating a family’s genealogy were powerful ways to rob people of the essence of their humanity. If enslaved people had no humanity, then you can justify enslaving them and depriving them of any rights. They are no better than property or animals (though antebellum “gentlemen” were careful to record the pedigrees of their race horses).
Family histories help societies and people make sense of their lives and the world they live in by telling a particular story. Every family history is a family story. But every story has a reason it is being told, one that determines the cast of characters, why they are included, and why some characters are left out. Some stories are noble, some mundane, some medical, some political, and some are religious. The darkest stories are those that oppress and those that cannot be told because they have been destroyed, taking with it the soul of a people.
Justin Lorentz is a certified genetic counselor who graduated from McGill University in 2012. He spent 8 years working in cancer genetics at Sunnybrook Hospital in Toronto, Canada where he developed an academic interest in prostate cancer genetics. He now works at Sunnybrook one day a week leading their Familial Prostate Cancer Clinic. Justin spends the rest of his time at Medcan, a Canadian preventive healthcare clinic offering proactive genetic testing, pharmacogenomic testing, carrier screening, NIPT, and healthy whole genome sequencing.
Two years ago, I saw the NSGC rebrand a pillar acronym for DEI initiatives into a pillar franchise: Star Wars, and more specifically, their JEDI. This was at a time when J for Justice was starting to be included in many Diversity, Equity, and Inclusion (DEI) committees. Most committees threw the J on the end. The NSGC did not, and on April 8th, 2021, the NSGC released an introduction to the J.E.D.I. Committee. The potential of the Star Wars franchise reference to trivialize the efforts of the committee was brought up in the publication, but the post argued JEDI is easier to say and through “listening and conversation with others” a vote was struck up with the committee to settle on their name: the J.E.D.I Committee.
And the NSGC was not alone. The American Association of Geographers, Big Brothers and Big Sisters of America, heck, The Canadian Psychological Association all have a JEDI, and many JEDI committees lean into it, lightsabers, and all.
But something about the J.E.D.I. acronym never sat right with me. I remember thinking, imagine if the letters DEIJ magically spelled out MUGGLE, and the NSGC’s DEIJ committee adopted the M.U.G.G.L.E acronym instead. What would happen to that committee’s name after J.K. Rowling would go on to make her TERFY statements on trans women? Rebranding DEIJ to a franchise is risky because you have no control over how that franchise’s brand can evolve. It’s begging for a PR problem. But even more so, what do Harry Potter and Muggles have to do with DEIJ or genetic counseling? If the answer is nothing, then the risk of rebranding DEIJ into something it isn’t is not worth it to me.
Over the years of seeing the J.E.D.I. acronym on NSGC updates in my Gmail inbox and on Twitter, my thoughts on the J.E.D.I. acronym for a DEIJ initiative started maturing. I debated whether my issues were worth publicly expressing until I came across this Scientific American article which summed up my growing concerns, and more.
After dwelling long enough I decided my need to express my opinion more loudly. I agree with the NSGC DEIJ Committee’s initial instincts that the J.E.D.I. acronym does trivialize the DEIJ Committee, but to me that just scratches the surface. When you dig but a little deeper, you realize that JEDI has its own meaning, a controversial history, and a diehard fan base. It not only distracts from DEIJ work, but I think the word JEDI opposes DEIJ work, not just for our professional organization, but for any organization.
There’s a lot to think about and you need to know about the Star Wars franchise to really put it all together. I realized this as I ran this DNA Exchange blog post by my partner, who has never seen media from the Star Wars franchise. Although it’s probably safe to assume most people attuned to Western culture know what a Jedi is, the more you learn about Jedi and their Order, the more problematic it all becomes as the title for any DEIJ work.
In case you’re someone who does not feel included in my previous assumption that most folks know what a Jedi is, let me sample Merriam-Webster to do the definition justice, so we’re on an equal playing field. *Nerd mode activated* Jedi are a very select group of monk-like galactic warrior/priests, both humans (the historic stars are white cis-gender males) and alien (Yoda), who are proficient with melee weapons called lightsabers. They’re all born with a seemingly inherited wealth of abilities including accessing and manipulating a spiritual/cosmic energy called The Force to perform supernatural feats like levitation and the famous Jedi mind trick (Eek! There’s NSGC J.E.D.I. Action Plan Task Force – How many other communications from the J.E.D.I. committee could/have become unintentionally conflated with trivializing aspects of the Star Wars franchise?).
Jediism, like Scientology, has made its way from the sci-fi world into the real world. In 2005 the Temple of the Jedi Order was registered in Texas and was granted federal income tax exemption by the IRS in 2015. The Church of Jediism purportedly boasts up to 500,000 members worldwide. Although faith is an important part of a patient’s values and decision making, the genetic counseling profession is not aligned or defined by any one faith, especially not this one. It’s a bit out there, but the NSGC’s J.E.D.I. Committee is sharing a brand with Jediism, even if it is in name only.
Let’s explore the idea of a PR problem further – what happens when the Star Wars franchise comes under scrutiny? More importantly, what if the scrutiny is DEIJ related?
Law and Philosophy professor Patricia Williams wrote a very compelling article called Racial Ventriloquism in 1999 after Episode I: The Phantom Menace came out. Here she highlights racist depictions of two alien characters from the Star Wars franchise: one popular, one more forgettable (until now).
Exhibit A) Jar Jar Binks: He’s a Gungan, an amphibious alien species with a frog-like face. He’s portrayed a little less clever than the average alien, panicky, having poor judgement, and being clumsy. He is the main source of comic relief and he and his species share a characteristic jovial, swaying saunter complete with a striking West African, Caribbean, and African American linguistic style. Patricia quotes a few phrases here to jog your memory if you haven’t heard him talk in a while: “You-sa Jedi not all you-sa cracked up to be.” “Me berry berry scay-yud.” “We-sa goin in da wah-tah, okeyday?”.
Exhibit B) Watto: He’s a Toydarian, a potbellied alien with insect like wings and a large nose like a tapir. He’s portrayed as a money-obsessed junk dealer and slaver. His accent seems Middle Eastern, and Patricia notes he bears eerie resemblance in shape and clothing to a cartoon published in Austria’s antisemitic Kikeriki magazine, right down to the hat.
These are two examples of many controversial aspects of the Star Wars franchise brought up over the twenty-four years since the release of Star Wars: Episode I – The Phantom Menace. Admittedly I forgot aspects of these controversies and it took researching them to realize the incredible depth of the problem. I’ll be honest, I wouldn’t expect anyone to be digging into the racial allusions the Star Wars franchise had made over 20 years ago when considering using J.E.D.I. in 2021, but now that we’re here I think we can all agree it’s hard to unsee.
And what about now? It’s not only the Star Wars franchise that’s racially controversial, but also some of its fanbase. Take the more recent racist backlash of Star Wars fans when the now Disney+ owned Star Wars franchise introduced Moses Ingram, a Black female Sith-like antagonist in the Obi-Wan Kenobi series released last year in 2022. Unfortunately, she’s not alone; other actors have faced similar racist attacks:
Ahmed Best (Black actor who played Jar Jar Binks) that was so persistent he contemplated suicide
Kelly Marie Tran (Asian actor who played Rose Tico) in The Last Jedi and The Rise of Skywalker
It’s debatable whether this reflects poorly on the Star Wars franchise per se, but what it does show is the franchise attracted fans who expect something of the franchise, fans who have their own preconceived beliefs of what they want lead characters in this Jedi series to look like.
How are we feeling after all of this? What are you thinking about right now? Are you seeing the word Jedi through a different lens?
I am.
For me, Jedi, and the Star Wars franchise that birthed Jedi, do not have a place in any DEIJ committee due to Star Wars’ bizarre religious movement, racial controversies, and certain members of their fanbase with strong opinions on the diverse direction the franchise is trying to tale. The word Jedi carries a lot of its own baggage and its own meaning.
To me, DEIJ means what it is: Diversity, Equity, Inclusion, Justice. It may not be easy to say, but neither is 2SLGBTQ+, and neither is challenging our own internal biases ingrained in us from a society built on systemic racism, sexism, ableism, and other injustices. Let’s keep DEIJ as its own important and well-established brand.
The initial reasoning for the NSGC DEIJ Committee to be called J.E.D.I. was fair for that time, and the NSGC’s newly forming DEI committee was not alone in their thought process. Knowing more at this time, I don’t think the NSGC’s J.E.D.I. Committee should continue calling itself something it isn’t. I hope the work of any DEIJ committee is nothing like the work of the Star Wars franchise or their Jedi. In fact, I feel Jedi go against DEIJ committee work. I want to see every DEIJ Committee for what it is, a hard to say acronym, making hard to do changes in what I think is one of the most important areas of development in our profession over the next few years. I think it’s time for a rebrand.
These are my thoughts – I’m interested to hear yours.