By: Rachel Hodan, MS, CGC on behalf of the Advisory Board of the Lauren Ryan Genetic Counselor Assess Memorial Award
Many readers likely knew Lauren Ryan, a beloved genetic counselor, colleague, and friend. Lauren embodied the tenets of genetic counseling in her intellectual curiosity, her work ethic, and her incredible empathy. She was multifaceted (heterogeneous I dare say?). She loved dogs and babies, burritos, and vegan food, could make a snarky comment when needed and she had horribly weak ankles. She once casually stepped off a street corner in San Francisco after we had lunch and ended up with bilateral twisted ankles.
Lauren graduated from the University of Missouri with a BS in Biological Sciences and a minor in leadership and public service. She was in the inaugural class of the California State University Stanislaus Genetic Counselor program and graduated in 2010. She was interested in moving to the Bay Area and energized by being part of something new. She harnessed this “first” mentality when she was hired as the first Genetic Counselor at Color Health, then a small Silicon Valley start-up. She built and managed a team at Color and then took a position at GRAIL in 2021 as a senior manager.
While she built her leadership skills, Lauren’s GC professional work also focused on supporting “any and all initiatives that would build a more diverse and inclusive community and increase equitable access to genetic counseling services”. Those are Lauren’s own words in her application to be a board member of the National Society of Genetic Counselors. She was elected to the NSGC board and was slated to serve starting January 2023. She tragically died in a car accident in December 2022.
Lauren’s list of volunteer positions through NSGC and beyond take up an entire column of her CV, including her incredible work on SIG committees, varied working groups and task forces, and she was recognized as NSGC’s 2021 Outstanding Volunteer Award recipient. She was passionate about supporting GC students and would always give of her time to prospective students for informational interviews or shadowing. Lauren was known for taking students randomly out for a free meal—acknowledgement of the practical needs of a student that may be overlooked. It was this support for students and our own profound personal grief, that led our small advisory group to develop the Lauren Ryan Genetic Counselor Access Memorial Award. The award is housed under NSGC’s non-profit The Genetic Counseling Foundation. The first planned award will be given in Summer 2025 to a rising 2nd year GC student, and we encourage those who are eligible to apply.
Lauren admired the field of genetic counseling, but she was also committed to its growth and improvement. The mission of the award is to increase access to the field of genetic counseling for traditionally underrepresented populations through financial support. We have had tremendous grassroots funding support, but we have not yet met our sustainability goal to allow for ongoing awards. We are achingly close! We would be so grateful if you would consider an individual donation or send us leads on additional corporate sponsorship. Tax-deductible donations to support Lauren’s legacy can be made here.
Any number of her friends could tell a meaningful story about Lauren. Here is one of mine: Lauren was the first person I told when I passed my board exam. Yes, these were the times before you found out immediately. I raced down the hallway to her office at the UCSF Cancer Risk Program and shouted so loud that multiple people came out to see what the emergency was. Lauren was jumping up and down with excitement for me, crying because I was crying, so full of joy and life and support and friendship. She was the best conversationalist you have ever encountered, and an absolute gem of a person. We miss you so much Laur.
Lauren Ryan GC Access Memorial Award Advisory Board
Mary Bloszies MaryAnn Campion, EdD, MS, CGC Elizabeth Duff Carrie Haverty, MS, CGC Carmelina Heydrich, MS, CGC Rachel Hodan, MS, CGC Carla McGruder, MS, CGC Cindy Morgan, MS, CGC Diego Quintero, MS Lily Servais, MS, CGC
‘Lauren was one in a trillion. She was beyond kind, compassionate, loving, and funny. She made everyone she met feel special and that they were worthy of time, attention, love, and taking up space in the universe. She loved animals and babies. She was an excellent dancer. She was incredibly smart and insightful. She was selfless while retaining a strong sense of self. She made the world a better place and she will be missed by everyone who knew her for the rest of their lives.’
“She truly embraced a spirit of inclusion whether meeting a person for the first time or the 100th time….She drew you in and spread her warmth and love.”
“Lauren was one of a kind. She created spark and energy with her very presence in any setting and had a way of drawing out the extra voltage in all of us to do more and live more fully…. If you asked Lauren for a favor, to give a presentation, to attend an event, or just about anything, she unhesitatingly would say “yes!”. In this day and age when everyone is so protective of their time, she magnanimously found time to give and live.”
I am in the midst of watching the Jeux olympiques d’été de 2024 (aka The Paris Olympics, the XXXIII Olympiad), one of the benefits of retirement. As I write this, Rowdy Gaines is narrating a swimming event with his usual infectious and unconstrained enthusiasm (every country has its own Rowdy Gaines equivalent for various sports). Watching the marvelous bodies and performances of these athletes triggered some thoughts about which bodies are or are not allowed to compete. More specifically, I began reflecting on the history of using genetic testing to determine which athletes would be permitted to compete in women’s Olympic sporting events. It’s a tale of how the inappropriate use of genetic testing can have far reaching ethical, political, legal, social justice, sexual bias, and racial bias effects.
There is wide agreement that elite biological male athletes generally have superior physical performances compared to elite biological female athletes in some sports. It is an understatement to say that evaluating athletes to determine if they are “female enough” to compete as women is highly controversial, including among athletes themselves. I am not going to enter that fray here. The problem is that biological sex is more of a spectrum than a duality.* The pegs of our bodies come in many shapes but the sports world – and society at large – tries to squeeze these multiform and at times changing pegs into either square holes or round holes.
They lined us up outside a room where there were three doctors sitting in a row behind desks. You had to go in and pull up your shirt and push down your pants. Then they just looked while you waited for them to confer and decide if you were OK. While I was in line I remember one of the sprinters, a tiny, skinny girl, came out shaking her head back and forth saying. ‘Well, I failed, I didn’t have enough up top. They say I can’t run and I have to go home because I’m not ‘big’ enough.
Genetics entered the picture when the IOC Medical Committee introduced Barr body testing into the mix in the 1960s. In 1949, University of Western Ontario researcher Murray Barr and graduate student Ewart G. Bertram published a paper in Nature in which they demonstrated that, by using a simple staining technique, the chromatin of a cell’s inactive X chromosome in individuals with two X chromosomes could be identified with a microscope. In a methodology that might be ethically questioned by some today, Barr used feline neural cells obtained by brain biopsies of anesthetized cats. As every student of genetics knows, one X chromosome stays active and the remaining X(s) is inactivated in individuals born with more than one X chromosome. And, as every student of genetics knows, Barr body analysis is a less than perfect indicator of biological sex. Nonetheless, the IOC chose to use this analysis to determine who could or couldn’t compete in women’s competitions. It was a relatively easy test to perform at scale using buccal cells or (ouch!) hair bulbs.
Starting with the 1968 Winter Olympics in Grenoble, the IOC randomly tested some female athletes using Barr body analysis and sometimes Y chromosome fluorescence studies. In the 1968 Mexico City games, Mexican geneticists Alfonso León de Garay and Rodolfo Félix Estrada organized a large scale genetic testing program of 1,265 Olympic athletes and perform a wide array of genetic, cytogenetic, and familial studies in an effort to study the determinants of athletic ability. Their analysis included karyotyping but those specific results were not made available so it is unknown if any athletes were disqualified and how many actually underwent sex chromosome studies. By the 1972 Sapporo games, genetic testing of female athletes became mandatory (except for Princess Anne, sister of Queen Elizabeth, who, when she competed in equestrian events in the 1976 Montreal games, was given a pass on undergoing sex testing). Barr body analysis +/- Y chromosome staining continued until 1992, when they were replaced with SRY and/or DYZ1 PCR studies. As with Barr body and Y chromosome studies, SRY and DYZ1 status are also less than perfect predictors of biological sex. Some athletes “passed” Barr body testing in one Olympics only to “fail” the PCR test in a later Olympics. Sometimes you were female, and sometimes you weren’t, depending on the whim of the the rule makers and the available genetic technology.
Official reports of the Olympics used various names to refer to these genetic tests over the years: sex checks, sex control, femininity tests, femininity testing, femininity control, gender verification, gender testing, gender tests, and sex checks. Sometimes names fell into disuse only to resurface years later. This illustrates how changes in language norms often do not follow a straight-line trajectory, as well as confusion about distinctions between sex and gender, and just what it is the rules were trying to get at.
It’s unclear how many individuals were excluded from Olympic participation based on sex verification testing because the IOC didn’t always reveal that information and they wished to protect the confidentiality of the athletes, but apparently very few athletes were actually excluded, even if they “failed” the tests. Of course, some athletes may have been excluded by testing in their home countries before they were allowed to go to the Olympic Games and some Olympians may have quietly bowed out before the start of the Olympics if testing at the Olympics didn’t qualify them as women. By 1999, the IOC abandoned mandatory sex testing.
There are more instances of exclusion based on sex testing in non-Olympic competition, several of which received extensive and at times sensationalized media attention. In particular, some athletes were identified with differences in sexual development , and these athletes continue to pose the most controversial, challenging, and contentious situations for sports regulatory committees, athletes, the media, and the general public. Some intersex athletes were unaware of their conditions prior to testing. It’s tough enough explaining this information within the context of a genetics clinic to someone for whom there was at least a suspicion of an intersex condition. Imagine finding out for the first time just before a major athletic event and then sometimes having that information broadcast around the entire planet. Some athletes experienced serious psychological problems as a result.
Some in the genetics community expressed concerns about the use of these tests almost immediately. The objections raised by Albert de la Chapelle, Malcolm Ferguson-Smith, and the Singapore pediatrician/geneticist Wong Hock Boon, among others, were largely ignored. The Social Issues Committee of the American Society of Human Genetics also issued a report criticizing the use of genetic testing in sports. It’s unclear how much these objections influenced IOC policies. The IOC seemed to react more to social and media pressure than the opinions of physicians and scientists.
The IOC abandoned mandatory sex verification in 1999 and after two decades of changing rules recently produced a more fair-minded and inclusive policy following the Tokyo Olympics in 2021. However, the IOC leaves it up to the governing bodies of individual sports to determine who can compete as a woman. Many of these individual governing bodies use athletes’ testosterone levels to determine eligibility, as does the Women’s National Basketball Association and the National Women’s Soccer League in the US. Thus athletes such as Mokgadi Caster Semenya, Francine Niyonsaba, and Christine Mboma have been identified as intersex, and in some cases have been told they need to to undergo ethically questionable medical interventions such as gonadectomy or testosterone lowering drugs to compete in certain events. This can take deep physical and psychological tolls on interesex and transgender athletes, the ones who probably suffered the most from sex verification testing in athletic competition.
The general justification offered for sex verification testing is to level the competitive playing field. That is understandable and many athletes likely support that general concept. Fair compeition is, after all, why performance enhancing drugs are banned. However it is interesting that genetic testing was only offered for X or Y chromosomal material. There has never been routine testing for autosomal genes, such as some alleles of the EPOR gene, which can give an edge in marathon type sports by allowing the blood to carry more oxygen. The Finnish cross country skier Eero Antero Mäntyranta won 7 medals in 3 Olympics, possibly aided by his diagnosis of primary familial and congenital polycythemia (ironically he later tested positive for amphetamine, a performance enhancing drug). Although all of the genes linked to athletic ability have not been identified and is likely the result a complex interplay of many genetic and environmental factors, I am pretty sure the genomes of LeBron James, Katie Ledecky, Diana Taurasi (one of the most complete basketball players I have ever seen), and Lionel Messi look different than a lot of their competitors’ genomes, not to take anything away from these athletes intensive training regimens. But we don’t classify athletes by genotype – unless of course that genotype is related to biological sex.
The misuse of complex genetic information also occurs in non-athletic situations – MTHFR polymorphism testing, polygenic scores calculated for IVF embryos, ancestry testing to justify white supremacy, to name a few. No matter how hard geneticists try to shape the public conversation about genetics, once the CATG is out of the genetic bag, we have very little control over how it is reported, used, and misused. It plays out in social, political, legal, and ethical landscapes in unpredictable and at times harmful ways. It’s not merely a matter of better education of the public and various authorities. How genetics and other scientific information is used is shaped by prevailing ideologies, politics, and diverse cultural values. And sometimes by narrow-minded hate.
_______________________________________
– My favorite example of the non-duality of life is the green sea slug,Elysia chlorotica. In its juvenile stage it is brown with white spots and looks like, well, a slug. It seeks out specific algae –Vaucheria litorea – for food, and sucks out the algal cell’s contents, including the chloroplasts. The snail no longer needs food at this point, getting all of its energy from photosynthesis via the algal chloroplasts it ingested. Not only that, it transforms its morphology such that it eventually has a slug head but its body color changes to green and looks for all intents and purposes like a leaf, complete with veins. I first learned about E. chlorotica in The Light Eaters, Zoë Schlanger’s fascinating book that will challenge your ideas about plant life. Oh, and by the way, along the lines of trying to define biological sex, a green sea slug produces both sperm and eggs.
Medical geneticists and genetic counselors have an often complicated and at times tense relationship with people with disabilities, their families, advocates, and scholars. Geneticists are strong advocates and supporters for all of their patients, regardless of their abilities and disabilities. Although people with disabilities should not be viewed as a homogenous group with no variation in attitudes and beliefs, a visit to a genetics clinic can make patients feel very “other” when they are analyzed, catalogued, measured, and examined to determine just how different they are, to find out what’s “wrong” with them. Many patients and advocates – though by no means all – view prenatal testing as an existential threat. To better understand this situation, a look at the historical origins of medical genetics can shed some light on this dynamic.
The medical genetics specialty began to cohere and develop in the decades between the 1940s and 1970s. Its roots go back before 1940, mostly in the form of eugenics. The term “medical genetics” was introduced in the early 1930s*, likely independently, by the eugenics-minded Madge Macklin, then at the University of Western Ontario, at the 1932 Third International Congress of Eugenics and in 1931 in the UK by the vehement critic of eugenics Lancelot Hogben in his text Genetics Principles in Medicine and Social Science (although he proposed his own eugenic ideas in the text). But there was no clear cut profession of medical genetics or providers who called themselves genetic counselors in the early decades of the 20th century.
Lancelot Hogben’s text where he introduced the term “medical genetics.”
P. 214 from the Hogben text
Madge Macklin’s paper in which she introduced the term “medical genetics,” apparently independently from Hogben. Presented at the 3rd International Congress on Eugenics, New York City, 1932. Note the first sentence of the last paragraph, which states: “Until the medical practitioner is made aware of heredity as an etiological factor in the production of disease, he will not be apt to have a sympathetic attitude toward public education nor toward any scheme which may be devised to curtail the heavy economic waste of caring for the hereditary defective.”
The formative period for the medical genetics specialty began shortly after WWII ended. The first medical genetics clinics opened their doors in the 1940s and 1950s. The American Society of Human Genetics, the first professional organization for medical and other human geneticists, was established in 1948; its flagship journal, the American Journal of Human Genetics, first began publication in 1949. Accurate human karyotyping,** the primary genetic laboratory test for decades, became available during the 1950s, thanks to the work of Tjio and Levan. Several foundational texts were published, such as Victor McKusick’s Mendelian Inheritance in Man in 1966, Dave Smith’s Recognizable Patterns of Human Malformation in 1970, and Josef Warkany’s Congenital Malformations in 1971. The American Journal of Medical Genetics began publication in 1977. The American Board of Medical Genetics (now the American Board of Medical Genetics and Genomics), the original professional certifying organization for medical geneticists and genetic counselors, was incorporated in 1980. These achievements are hallmarks of a nascent profession working to establish its professional scope and legitimacy. They resulted in the creation of jobs, hospital departments, clinical laboratories, a research tradition, the profession of genetic counseling, and eventually contributed to the expansive growth of prenatal testing and commercial genetic testing laboratories.
Historians of science have offered several explanations for this post-WWII growth, such as increasing sophistication of genetic knowledge, an ethical reckoning with eugenics, advances in medical technology, and epidemics of teratogenically-induced fetal conditions such as fetal rubella syndrome and fetal thalidomide syndrome in the 1950s and 1960s. While these were contributing factors to the formation of the Medical Genetics specialty, I would argue that they were secondary rather than primary factors. Medical genetics was built primarily on the minds and bodies of people with genetic and congenital disabilities. Disability – and social attitudes toward it – was the initial raison d’être for medical genetics and the associated genetic counseling. Of course geneticists saw patients for indications other than disability. For example, a very common reason for referral to genetics clinics was to try to determine the ultimate racial appearance of an infant up for adoption so that it could be placed with a “racially appropriate” family. But the primary clinical focus of the early genetics clinics was the clinical evaluation of people with disabilities. No disability then no medical genetics (or at least a medical genetics that would have looked very different).
How can I make such a claim? Well, during this period there wasn’t much in the way of treatment for most genetic conditions. Instead, geneticists focused on describing the bodies of people with disabilities in painstaking clinical detail. Naming and identifying syndromes and their differences and sub-types. Determining the likelihood of a condition occurring or recurring. Describing anatomical structures that have gone embryologically awry. Measuring the distance between the eyes, the length of the philtrum, the distal phalanges, the head circumference. Noting the angle of the palpebral fissures, the insertion of the ear, the location of the anus relative to the genitalia. Commenting on the presence or absence of a single palmar crease, soft tissue webbing, fifth finger clinodactyly. How the bodies of people with disabilities were dysmorphic, malformed, deformed, and disrupted. In short, how their bodies differed from the “norm.” This gave medical geneticists a common vocabulary with which to communicate with one another, unique clinical skills, and it provided scientific legitimacy to their efforts. It also undoubtedly didn’t make people with disabilities feel good about their bodies. Nor would the stark clinical photographs published in genetics books and journals that sucked the dignity and humanity right out of the patients (often pictured naked and with their eyes blackened out).
This approach to patient care allowed the first waves of medical geneticists to establish their clinical expertise and carve out a professional niche that set them apart from pediatricians, neurologists, and other medical specialists. No other branch of medicine focused so heavily on parsing out human macro- and micro- phenotypic variation. A medical specialty was born.
Every medical specialty has its clinical focus, usually defined by specific diseases or organ systems. Oncologists treat cancer patients. Nephrologists care for patients with kidney disease. Cardiovascular specialists manage patients with heart disease. These patients were regarded as “normal” people with unfortunate diseases that needed to be treated and cured. People with disabilities were regarded as unfortunate people who needed to be prevented, reflecting prevailing social attitudes of this period. The genetic counseling provided during that time echoed these attitudes. Despite disavowals of eugenics, post WWII genetic counseling focused on avoiding the births of disabled bodies.
This is not to imply that medical geneticists during this period were bad people who intentionally and callously used the bodies of people with disabilities for personal and professional gain. These men (and they were almost exclusively males) were for the most part kind and compassionate physicians who cared deeply about their patients and usually treated them with respect and dignity, just like almost every medical geneticist I met throughout my career. Many patients were very grateful for the care they received in medical genetics clinics. It wasn’t a matter of bad physicians providing sub-standard medical care for devious purposes and personal gain. Rather, medical genetics was an outgrowth of the ableist and anti-disability structure of medicine and of society as a whole.
There was of course some level of reciprocity. People with disabilities and their families could benefit from the services provided by medical geneticists. A syndrome name to help end the Diagnostic Odyssey. Anticipatory medical and developmental guidance, referrals to neurologists, surgeons, educators, physical therapists, and other specialists who might treat and care for patients’ often complicated medical issues. A medical home where patients could make sure their often complex medical needs were being tended to and coordinated by a single care provider. An expert authority who could provide education and knowledge about often rare conditions that were beyond the clinical knowledge of pediatricians and other non-genetics providers. But the benefits were asymmetric. Patients and their families came away with perhaps recurrence risks, maybe a syndrome name, and some idea of what their medical and developmental futures might look like. But people with disabilities have managed to survive and live their lives since the dawn of humanity (though now always pleasantly) without the existence of medical geneticists. Medical geneticists, on the other hand, gained an entire profession. They needed the bodies of people with disabilities in order to create careers and a brand new medical specialty.
Medical geneticists today still care for patients with disabilities, though the situation is more nuanced and complex than in the past. Patients are generally treated with greater respect and have greater autonomy. Medical geneticists and genetic counselors have expanded their scope of practice to conditions beyond disability, such as cancer, neurological disorders, cardiovascular diseases, pharmacogenomics, and psychiatric conditions. Social attitudes toward disability are less negative than they once were and this is reflected in the way genetic counseling is provided. Genetic analysis has become more sophisticated. There are more treatment and management options for the health problems associated with genetic conditions, helping some people with disabilities and their families lead richer, healthier, and fuller lives.
Nonetheless, the historical tensions persist. Patients and providers often have different views of what constitutes a disability and what disorders need testing, treating, and curing. The list of conditions amenable to prenatal testing grows exponentially, usually with little or no input from the people and families affected by the conditions. The value of people with disabilities is often still measured in economic terms. Structural, conscious, and unconscious ableism is ubiquitous, even among the most sensitive and supportive providers and institutions. We’ve come a long way, but it’s still a long haul to go.
___________________________________________
* -The Macklin and Hogben references were the earliest I could find on the origin of the term “medical genetics.” If readers are aware of earlier references, please let me know.
** – Human, plant, and drosophila chromosomes had been analyzed since the early decades of the 20th century. However, the crude laboratory techniques did not always allow for accurate analysis or even correct chromosomes counts. The word karyotype was coined by the Soviet plant geneticist Grigory Livitsky around 1930. Like many Soviet geneticists of the Stalin era, Livitsky was arrested and eventually died in a Soviet prison in 1942 after ideological clashes with Stalin’s favored geneticist, the notorious Trofim Lysenko. Lysenko rejected Mendelian genetics and his scientifically misguided agricultural policies led to catastrophic crop failures, widespread famine, and millions of deaths in the Soviet Union and China, which also followed Lysenko’s lead. As with the Covid pandemic, millions of avoidable deaths resulted from a rejection of sound science and research.
In this post, the word “fat” is used intentionally to follow the language of fat advocacy organizations. This is meant to challenge the notion that the word “fat” is inherently bad but rather is a neutral descriptor that describes the bodies of many people. As with other identities, individuals may prefer the use of other terms to describe themselves, in which case it is always best to mirror that language.
Genetics is at the core of many efforts to address the “obesity epidemic.” Genetic tools such as polygenic scores, CRISPR-Cas9 technology, and direct-to-consumer genetic tests share the goal of minimizing fatness. Not only do these efforts ignore the already understood social determinants related to weight and health, but they consistently exclude the perspectives of fat people. Additionally, gene panels designed to identify monogenic causes of obesity raise concerns; while they might be able to provide actionable medical information, the focus should not be exclusively on weight loss.
When we center weight loss as the main mechanism to support one’s health, we reinforce the persistent idea that if someone is fat, they are, by definition, unhealthy, and addressing their weight, therefore, must be a top priority. This can lead to experiences where people’s health concerns are not taken seriously or further explored, perpetuating mistrust in the healthcare system and subpar care. As the genetic counseling profession strives to promote more inclusive and equitable spaces, it is important for us all to reflect on our own biases and minimize over-pathologizing fatness.
Anti-fat bias is pervasive
Fatness is unique in that it is both externally visible and it remains socially acceptable to point out or express dislike for. One’s weight is often attributed to a direct depiction of a person’s character or behavior. Fat people are seen as “lazy” and “lacking willpower,” while thin people are perceived as having “earned” their societal advantage. In her book Hunger, Roxane Gay writes,
“When you’re overweight, your body becomes a matter of public record in many respects. Your body is constantly and prominently on display. People project assumed narratives onto your body and are not at all interested in the truth of your body, whatever that truth might be. Fat, much like skin color, is something you cannot hide, no matter how dark the clothing you wear, or how diligently you avoid horizontal stripes” (page 31).
Media reinforces these beliefs. Popular films and TV shows such as Super Size Me and The Biggest Loser present opportunities for viewers to pass judgment on those who engage in “fattening behaviors” while further solidifying one’s pre-existing belief that thinness is earned by a series of correct decisions. Even in the recently released Wonka, fatness stemming from gluttony, selfishness, and poor morals is used repeatedly as a punchline. News coverage of the so-called “obesity epidemic” is filled with unflattering images of “headless” individuals, often sedentary or eating “unhealthy” food. Imagery such as this works to remove the humanity of people who are fat and further the widespread belief that fatness is simply a result of “bad choices.”
Similar to other forms of oppression, people experience anti-fat bias in many ways. For example, there currently exists no federal protections and very few state protections against weight-related discrimination in the workplace. Fat people are often the subject of undesired critiques of their bodies, typically said under the guise of “caring about their health.” No space may be more dangerous for fat individuals than healthcare, where weight is weaponized against patients by providers claiming to “do no harm.”
While the relationship between health and weight is tenuous, there is a clear relationship between anti-fat bias and adverse health outcomes, including increased stress levels and healthcare avoidance. When individuals seek care, the quality of care they receive is often lower. For example, when seeking cancer screening as a person who is fat, there are many barriers, including providers who will deny services such as a Pap smear based on weight. Additionally, there is a history of the medical system causing harm through the over-prioritization of weight loss. One such example is that of Fen-Phen, a combination weight-loss pill that was eventually recalled due to it causing valvular heart disease.
Increasing accessibility to genetic counseling for patients who are fat
Genetic counselors provide support for individuals navigating healthcare spaces. Even though someone’s weight is not the indication for an appointment, people who are fat do not come to us in a vacuum. Rather, we fit into their broader experience seeking healthcare, which often includes experiences of bias and stigmatization. We must understand these experiences to provide adequate support and mitigate additional harm.
Genetic counselors must examine how to make their practices more inclusive for fat people. Are the chairs narrow and with arms, which may be uncomfortable for someone who is fat? Is there utility in taking the weight of the patients you see for your appointment? How is weight used in cancer risk assessment models? Are you making assumptions about someone’s health-promoting behaviors based on their weight? How do you discuss healthy diet and exercise? How are you discussing and recording no-call cfDNA results, challenges with ultrasonography, or limitations of standard MRIs being able to accommodate some people’s body size?
We also must be mindful of our language. For many fat people, the common-in-healthcare descriptor of “obesity” often evokes a negative response and feels overly medicalized. The term obesity is also a direct reference to the Body Mass Index (BMI), an ineffective predictor of health with racist origins and uses. Similarly, avoiding the use of phrases such as “struggling with their weight” to describe people can help mitigate the idea that being fat is inherently something one struggles with.
For decades now, fears of the “obesity epidemic” have harmfully implied that a person’s fatness is inherently detrimental to society at large. Over time, these ideas become so ubiquitous that people rarely question them. As genetic counselors dedicated to providing unbiased and supportive care to all of our patients, we need to understand the importance of unlearning and reflecting on systems of oppression, and anti-fat bias must not be an exception.
Sarah Wiser, B.S. (she/her) is a second-year genetic counseling student at Boston University Chobanian & Avedisian School of Medicine. Sarah is passionate about promoting equitable access to genetic counseling services and challenging anti-fat bias in healthcare.
This spring we will welcome a record number of new genetic counselors to the field. Based on 2022 year Match data from the National Matching Service Inc, we expect >500 new graduates in 2024.* The growing number of graduates is the natural result of more training programs and expanding class sizes in existing programs.
Unfortunately, it seems that this record number of new grads arrive to one of the worst job markets for genetic counselors in many years. Based on conversations I have had with a number of recent or soon-to-be genetic counseling graduates and informal conversations with several genetic counselors involved with training program administration, many new grads are having a hard time finding that first position. It is really tough for job seekers right now.
I am writing this to provide some historical background about why we might be in this position, and where we have so missed the mark in terms of supply and demand. It is my hope that we can learn from these mistakes and make changes as a profession to improve job opportunities, growth and security while also improving genetic services.
I am also writing though because I want to give assurance to all those entering the field in 2024 that it will get better. When I graduated, 20+ years ago I came out of my training program without a job, and I know how devastating and heavy that can feel. The job market has waxed and waned in the past and the pendulum will swing the other way at some point. The reason for my optimism is that, although our current job boards don’t reflect this, I believe that now, more than ever there is a need for the expertise and services that we can provide as genetic counselors. I want to reassure you that you will one day find that perfect job. And I also want you to know that the fact that you don’t yet have a job yet is not your fault.
How did we get here?
Recent history provides context for how we got to this point. Just over a decade ago, three major events rocked the field of clinical genetics:
Although it is hard to believe that there was a time before next generation sequencing (NGS), Sanger sequencing was the standard for many years. NGS allowed for gene sequencing to be done more cost-effectively and around 2010 we started seeing more multigene panels come to the market.
In late 2011 the first prenatal cell-free fetal DNA screening test, MaterniT21, became commercially available through Sequenom. In the years that followed, versions of cfDNA tests were released by multiple companies, creating an intensely competitive commercial landscape.
In June of 2013, Myriad Genetics lost their monopoly on BRCA1 and BRCA2 testing when the U.S. Supreme Court ruled that human genes could not be patented in the landmark case, Association for Molecular Pathology v. Myriad Genetics. This opened an opportunity for many labs to enter the genetic testing market.
All of these factors contributed to an enormous growth of the genetic testing industry and rapid escalation in demand for genetic counselors. The commercialization of the field of genetic testing was unlike anything we had seen before. Genetic testing was front page news and investors were lining up to be a part of it. Labs, flush with venture capital money, created many new job opportunities for genetic counselors.
In some cases, the job creation was very direct, with labs hiring genetic counselors as medical science liaisons, or to work in variant interpretation, product development and direct patient care roles. In other cases, the jobs created were with the telehealth companies labs hired to provide genetic counseling support to providers and patients ordering their brand of test. Additionally, the growing availability of genetic testing and investment in genetic testing technology created jobs in hospitals, clinics and research settings.
By 2015 it was clear that the demand for genetic counselors exceeded the number of trained people to fill the jobs. The following data was presented at the National Society of Genetic Counselors Annual Conference in 2015:
This graph contrasted the number of job postings on the NSGC job board with the number of genetic counselors coming out of training programs. In 2015, we had 291 genetic counseling program graduates compared to 655 job postings.
I am sad to say that this year, with ~500 graduates, there are 44 jobs listed on the NSGC job board at the time of this writing, and about half of these are not listings for genetic counselor jobs. In part, this reflects the fact that companies are not using the NSGC job board as their one and only means of recruitment, but it is also, undeniably, an indication that there are not many open jobs right now.
In 2015, a Workforce Working Group (WFWG) was established comprised of representatives from the American Board of Genetic Counseling (ABGC), the Accreditation Council for Genetic Counseling (ACGC), the Association of Genetic Counseling Program Directors (AGCPD) and the National Society of Genetic Counselors (NSGC). The charges to the WFWG were as follows:
● Identify current and future barriers and opportunities that impact the growth of the CGC workforce.
● Make recommendations to and support the development of specific action items that will facilitate growth of the profession and minimize and/or remove barriers to expansion.
● Drive and coordinate the efforts of the professional genetic counseling organizations to ensure the action items recommended by the working group are carried out in the most efficient and effective manner possible.
The WFWG commissioned a consulting firm, Dobson DaVanzo & Associates, LLC, to conduct a workforce supply and demand projection study of certified genetic counselors in the US over the time period from 2017-2026. This report considered many factors as they attempted to project the future needs and factors that could complicate their estimations.
The report developed two models in which the projected need for genetic counselors was 1 per 100K or 1 per 75K population and they projected we would reach equilibrium for the 1 per 100K model by 2026. While the workforce study recommended expanding existing training programs and developing new programs, they warned, “activities around this initiative will be focused on accelerating growth, while being mindful of not overreaching and exceeding demand.”
The report also raised concern regarding a “substitution effect” which was defined as other healthcare providers providing genetic counseling to patients. Additionally, the Dobson DaVanzo report also cautioned, “policies that restrict reimbursement to direct patient care by certified genetic counselors who are not affiliated with a commercial laboratory would likely reduce the effective demand for care, while at the same time reducing the ability of providers to meet patient need.”
This workforce report provided guidance on the importance of cautious growth with the caveat that it was an uncertain and rapidly changing landscape. The current situation has left me questioning if our profession considered this report in full as we have grown our workforce?
We met the Dobson & DaVanzo report’s projection of ~6.5K certified genetic counselors in March of 2023, more than 3 years ahead of schedule, and we continue to have more genetic counselors graduating from training programs than ever before. It does not appear to me that we have been “mindful of not overreaching and exceeding demand.” Of the 55 programs listed on the ACGC website, 14 are designated “new accredited programs”, and there are an additional 6 applications for programs in the works.
The substitution effect was defined by Dobson & DaVanzo as non-genetic counselors doing genetic counselors’ work. For the most part, we have not seen nurse practitioners, physician’s assistants or other providers stepping in to do the work of genetic counselors. From my view, what we have seen is that we are increasingly substituting ourselves. Let me explain. The labs understand that to compete in this market, it is essential to package genetic counseling with genetic testing. I see the labs going to providers who are neither equipped to nor interested in doing the counseling themselves, and offering complimentary genetic counseling as a perk for those ordering their brand of testing. The problem is, in many cases, genetic counseling provided gratis by a laboratory is not comparable to what would have been provided by a non-lab-affiliated genetic counselor in a clinical setting. The patient may get a message through a portal that tells them they can schedule a genetic counseling appointment. They may talk with a genetic counselor by phone for a few minutes to review results. What they rarely receive in these encounters is the comprehensive genetic counseling care that was factored into this workforce study. At this point, many providers and patients believe that this test-bundled follow-up care is standard genetic counseling. And, used to getting it for free, many providers and healthcare systems are now unwilling to pay what it costs to have genetic counselors on staff.
As important as it is, our profession has largely ignored the issue of how we are paid. This not only affects our job prospects, it affects the level of care we are able to offer to our patients.
The genetic testing lab bubble that began around 2013 created jobs funded by easy access to business loans and venture capital. Labs could use their huge investor funds to pay nice salaries to genetic counselors even when their companies were losing millions (and in many cases, hundreds of millions of dollars a year). The workforce study was developed at the time of this bubble and did not take into account the possibility that this job creation was unsustainable. Now, the VC bubble is deflating. After a decade of sustained and significant losses, investors are no longer willing to keep these labs going without return on their investment. Borrowing money has also become increasingly expensive and difficult. As a result, we are seeing labs retrench, close or be absorbed by competitors, with resultant layoffs of genetic counselors. And with many in our field looking for work, we have yet to reckon with the fact that we still don’t have a viable and sustainable funding model for genetic counseling services – in large part because fair reimbursement is difficult to demand when some version of genetic counseling services have so often been given away for free.
Another bit of history, and one the WFWG could not have factored in, was a global pandemic. Undoubtedly COVID-19 disrupted healthcare in ways that affected genetic counselors. As to the big picture, I think one important issue connected to the pandemic has been some of the financial challenges faced by many industries. For example the interest rate hikes, which have been a tool used to try to curb inflation has made funding more expensive and difficult to secure. The timing of this is unfortunate given the recent position of the labs. However, this does not change the fact that growing a profession on the basis of borrowed funds and start-up investors put us in a precarious place even without the added financial challenges brought on by the pandemic.
What comes next?
Given all that has changed over the last decade, and because we are nearly at the end of the period that the Dobson DaVanzo study had projected, I hope the WFWG has plans for another workforce study. Our profession is in need of an updated analysis of workforce issues.
Until we find a way to fund genetic counseling positions that does not rely on the house of cards that is laboratory funding, we should be mindful that our program growth does not outstrip the job opportunities for our newest colleagues.
The rapid growth in training programs suggests that the institutions involved looked at the rosy growth projections and ignored the recommendation to proceed with caution. Between the challenging job market and the difficulty securing clinical training sites for students, I imagine many involved in training programs are alarmed. While we have added many training slots, the program I attended, at Brandeis University, closed at the end of 2022 because there weren’t enough clinical training sites to serve the number of enrolled students the school required to cover the costs of maintaining the program. More programs may soon be facing tough decisions like this. One program director I spoke with shared, “many programs do not receive any state funding which means they have to run completely on tuition dollars. Even one student difference can break a budget that relies on those tuition dollars and may result in a program closing.”
In addition to considering carefully the growth of our profession through the training programs it is imperative that we all continue to advocate for fair reimbursement. The work we do as genetic counselors is valuable and crucial to the ethical practice of genetic healthcare, now more than ever. And I expect the need will only grow from here. But, we risk not being able to be in these roles, providing care and expert guidance if we do not first ensure that we have sustainable reimbursement for our services. Every single one of us needs to advocate for the “The Access to Genetic Counselor Services Act” so that genetic counselors are recognized by Medicare and can be reimbursed for the services we provide. This is everything. Have you contacted yourrepresentative?
I also hope we can mobilize as a profession to advocate for comprehensive standards of care in our work as genetic counselors. We should reflect on the recent challenges and disruptions we have seen in the field and consider how we are defining the practice of genetic counseling. If we continue to allow the profit motives of the labs to push us to act more as genetic testing facilitators, we will have an increasingly difficult time sustaining our ability to provide comprehensive genetic counseling and support.
Lastly I would like to send a message to all of the new and soon to be graduates who do not yet have jobs secured. Please don’t lose hope. You are the future of our profession, and we need you to help move us and genetic services forward for the better.
*The original version of this article stated, “A report published in 2022 by the Accreditation Council for Genetic Counseling (ACGC) indicates that ~800 genetic counselors will complete their training at the 55 accredited training programs.” and referenced the following report: https://www.gceducation.org/wp-content/uploads/2023/06/ACGC_2022_AnnualReport.pdf This was changed to reflect data from the National Matching Services Inc statistics, which reported that 547 applicants matched with a GC program in 2022.
A guest post by Ambreen Khan and Kimberly Zayhowski
Normative standards of professionalism dictate that a professional should remain apolitical, positing that separating personal beliefs from professional endeavors allows one to maintain objectivity. The enforcement of these standards is increasingly evident in genetic counseling spaces, such as with censorship in workplace meetings, on discussion forums and social media, and at conferences.
However, remaining apolitical grows complex given the politicization of everyone’s identities and personhood. The intertwining of personal, political, and professional realms is undeniable, often operating subconsciously. Operating in a makeshift bubble of neutrality disconnects us from the lived realities of our colleagues and the patients we strive to serve.
Eugenics underpinnings in genetic counseling
The roots of the genetic counseling profession are entangled with a history steeped in eugenics, a movement advocating for selective breeding to enhance the human population by using erroneous assumptions about genetics shaped primarily by social, political and personal biases of its supporters. Originating in the late 19th century, eugenics principles guided the atrocities committed during Nazi Germany’s reign, heavily shaped by American eugenicists like Charles Davenport and studies from the Eugenics Record Office at Cold Spring Harbor Laboratory. The historical justification of eugenics to forcibly sterilize, criminalize, and perpetrate genocide against minoritized communities has been rooted in the misappropriation of genetic and medical concepts. Therefore, dismissing the importance of politics in the field of genetics is a fallacy.
Genetic counseling’s origins can be traced back to the ethically fraught ideology of breeding out those considered less “desirable.” The justification for establishing and funding the first genetic counseling program suggested that genetic counseling serves as a strategy to mitigate hereditary diseases and encourage individuals to make informed decisions regarding reproduction, both for their own well-being and that of the broader population.
Despite the prevailing belief among genetic counselors that we are staunchly anti-eugenics, traces of eugenic ideology persist within certain aspects of our practice, aligning with broader political and power structures. This is exemplified by the recent NSGC Practice Guidelines suggesting the use of expanded carrier screenings as a means for downstream cost-savings through the prevention of births of individuals with certain genetic conditions.
Moreover, genetic counselors’ desire for absolute neutrality ties closely with the need to adopt a non-directive approach with patients, obscuring the intrinsically directive nature of everything said and done in patient interactions. This connectioncan be traced back to post-WWII geneticists’ efforts to distance themselves from eugenics, despite perpetuating comparable ideologies under the guise of neutrality. The norm to remain apolitical perpetuates self-censorship, impeding the field’s ability to openly confront its connections with eugenics.
The impossibility of neutrality
Acknowledging personal political beliefs becomes a crucial aspect of a genetic counselor’s professional journey and our interactions with colleagues. As Lewis Wallace, a transgender reporter, asserts in his piece titled “Objectivity Is Dead And I’m Okay With It,” neutrality is not real, particularly for people with marginalized identities who cannot remain neutral or centrist in debates concerning their own humanity. Hence, the structures demanding neutrality in the face of oppression must be challenged.
Numerous contemporary policies, such as those regarding immigration, disability and reproductive rights, racial justice, education, LGBTQIA+ rights, colonialism, imperialism, and more, directly impact how we show up in our professional lives. Policies can impede our capacity to pursue a career, such as when they impact visa status, restrict access to safe and inclusive work environments, or perpetuate discriminatory practices such as anti-transgender legislation.
The politicization of religious and ethnic identities to justify violence exposes individuals to bigotry, threatening their safety and sense of belonging. Politics can profoundly affect mental and physical well-being, as evidenced by US-funded genocide in Gaza and settler colonial violence in the occupied West Bank, leading to distress and safety concerns among Palestinian genetic counselors as well as allies that speak out against these atrocities. In such instances, neutrality serves oppressors, demanding marginalized individuals to suppress their emotions and well-being to conform to “professionalism” standards, which expect silence amid oppression.
The burden of representation and palatability
Standards of professionalism carry oppressive ideologies favoring white supremacy. Professionalism traditionally reflects the cultural norms, behaviors, and traits of the dominant social group, often represented by straight, cisgender, non-disabled white men in the broader field of medicine in the US, or women in genetic counseling. Consequently, professionalism tends to be assessed primarily among those who are racially minoritized, queer, gender-diverse, and disabled. An expectation of professionalism entails the ability to collaborate with others – even if those people say and do awful things. This creates an environment of dealing with microaggressions and discrimination quietly and laying low when witnessing bigoted conversations.
In navigating political dynamics, genetic counselors often encounter challenges with colleagues tied to respectability politics, a phenomenon where individuals from marginalized groups feel compelled to conform to mainstream expectations to gain social acceptance. Additionally, the pitfalls of “whataboutisms” arise, deflecting from the core issues at hand by pointing to separate problems or situations. This tactic often undermines meaningful discussions about systemic problems, diverting attention from the pressing need for change.
The pursuit of “palatability” within diversity, equity, and inclusion work can paradoxically prioritize the comfort of the oppressor over meaningful progress. Efforts to make conversations or initiatives more palatable risk diluting the urgency and discomfort inherent in addressing systemic issues. Individuals with minoritized identities often find themselves assuming the role of ambassadors for their communities. As they navigate professional spaces, they become de facto representatives, sharing the responsibility of dispelling stereotypes and fostering understanding. This burden is a consequence of existing in spaces where diversity is limited.
Integrating our personal, political, and professional selves
True progress in social justice work demands confronting challenging truths, dismantling entrenched power structures, and prioritizing the voices of marginalized communities over the comfort of those with privilege. Achieving this necessitates a deep understanding of one’s own privileges through an intersectional lens.
Without reflecting on the underlying reasons that necessitate our need to maintain objectivity while upholding the status quo, genetic counselors jeopardize their ability to engage in nuanced conversations with colleagues and patients. Staying engaged in global affairs is essential for genetic counselors to confront their personal biases and improve patient care.
Trusting ourselves and our colleagues to bring their authentic, political selves to professional spaces promotes meaningful dialogue and mutual understanding. The myth of apolitical neutrality acts as a barrier to recognizing the complexity of human experiences among colleagues and within ourselves. As we navigate the paradox of remaining apolitical in a world where identities are inherently political, genetic counselors must consistently question the root cause of their need for neutrality.
The opinions expressed in this article are solely our own and do not reflect the views and opinions of our employers.
Authors:
*Ambreen Khan, MS, CGC (she/her) works as a laboratory genetic counselor and a grassroots community organizer. A bilingual Muslim individual of Pakistani descent, Ambreen follows her passion of increasing access to equitable genetic services locally and globally, through educational talks, social media content, and research.
*Kimberly Zayhowski, MS, CGC (she/her) works as an assistant professor and research genetic counselor. A queer and multiracial individual, Kim is dedicated to advocating against oppression in genetic counseling research, education, and practice.
*Names in alphabetical order. These authors have contributed equally to this work.
As a rare disease genetic counselor – who both has a rare genetic condition and serves rare disease patient populations as a provider – I have a Rare Disease Day Public Service Announcement for you: Do not order Direct-to-Consumer testing and please actively discourage other providers and patients from ordering it themselves. We need to step up as a field and take a stance.
As a genetic counselor and patient in the rare disease world, every single week I’m being asked a question about these new “direct-to-consumer” genetic testing options. It can feel like whack-a-mole, with a new company or test being asked about every month. The second you feel like you understand most of the companies offering direct-to-consumer testing – you learn about another new company you’d never heard of.
Direct-to-consumer (DTC) genetic testing is any genetic test that can be ordered directly by an individual/patient from their home without the involvement of a medical provider with a trained medical director reviewing and signing off on every report. While some of these companies claim a medical provider has “reviewed all orders,” if the patient hasn’t had an appointment with said provider – then they are really just a rubber stamp on all orders. Why is that a key detail? The providers that work for, or are contracted by these labs, are reviewing these orders because of a regulatory loophole. They have every incentive to get the lab’s brand of testing paid for whether or not it is a test that is in the patient’s best interest. These providers do not have the time, or enough interaction with the patient, to truly assess if the test (or any) is the best fit for the patient and will answer the questions they have. A provider that is not affiliated with a testing lab needs to meet with patients for pre-test counseling so they can provide a nuanced conversation for informed consent, discussing the benefits and drawbacks of proceeding with genetic testing.
They may call it Direct-to-Consumer testing but it is more like Direct-to-Chaos testing, with “answers” that lead directly to false negatives, false positives, false promises, and patients with more questions than they started with. Except now patients have a scary list of potential conditions they’re being told they may have, but that healthcare providers can not (or should not) be using the “results” of, for diagnosing or treating symptoms. And I say this from experience – I have sorted through dozens of individuals’ “reports” from these websites and have looked up over 1,000 variants one by one. And what have I found? Not a single answer an individual was looking for. Not a single actionable result that was confirmed. In patients who have had multiple tests done by various DTC companies, almost never are the same “pathogenic” variants even reported by all of them, let alone also identified in the genetic testing they’ve also had done through legitimate labs.
Many say they’re offering whole genome sequencing but often what they provide is a whole lot of meaningless data with zero context, and interpretations that are inaccurate and misleading. As a genetic counselor who has a genetic rare disease these companies don’t just make me frustrated due to misinformation, they make me furious. They advertise something that’s too good to be true: a single test to look at all of your DNA, testing for every condition, at a fraction of the cost of a real medical genetic test. Why is this test so much cheaper? Because they’re essentially providing a giant data dump onto people. No quality control. No interpretation. Just big data grabs from the internet that result in false positives and negatives, and typically cannot even answer the question that the patient is asking.
“As a genetic counselor who has a genetic rare disease these companies don’t just make me frustrated due to misinformation, they make me furious.”
They purposefully target vulnerable families with unethical claims(advertising testing on infants), in order to draw individuals in by using all the right terms to mimic real testing, while carefully leaving out all of the caveats. There is a reason genetic professionals have ethical guidelines about not testing infants for adult-onset conditions. Somehow these companies are allowed to slide by as “just for fun,” while simultaneously providing individuals with lists of literally hundreds of “positive findings” for conditions such as amyotrophic lateral sclerosis (ALS) and BRCA1/2. “Positive findings” that in many cases are easily proven to be normal variation by checking free, public databases. How they get away with telling a patient they have a BRCA mutation and an 80% chance of breast cancer, when the variant is seen in over 99% of healthy controls (i.e. is normal variation) is astounding.
As a rare disease patient, I understand that it is beyond agonizing to be stuck on the “diagnostic odyssey” (which I prefer to call the undiagnosed purgatory). Going through 4-10 years of specialists with endless invasive and expensive tests. Being told by provider after provider that your symptoms are either A. all in your head, B. caused by stress, or C. would go away if you could just lose weight – of course families are desperate for answers. So when a website offers a single test to cover everything – it sounds like it’s worth spending a couple hundred dollars to finally get help. What they don’t say is that they’ll provide dozens of pages of useless, misleading information that even a trained genetics professional would take an entire week to sort through. My greatest achievement from hundreds of hours of work trying to pull something useful from these results? Talking individuals out of the extreme anxiety the false positive results have provided.
Sure, some of the DTC companies are easy to weed out as garbage (such as the ones offering a promiscuity genetic test). But I’ve talked to parents who did “whole genome sequencing” DTC testing on their dying child, hoping that somehow this data would be useful one day – not realizing that they heartbreakingly wasted their last chance at testing, such as banking DNA to do an actual medical grade test. I’ve talked with individuals who work in cytogenetic labs who have spent months combing through their data – who describe the “risk scores” provided by these companies as “a horoscope at best.”
The companies that sell these tests often have a disclaimer about these results only being “for fun” or “recreational,” however have in bold all over their website and advertisements the medical conditions that they claim they can test for with their “medical grade clinical test.” They know what they are doing – purposefully targeting families desperate for answers with social media campaigns, emails, and free giveaways of their product. The hard part is, when they provide literally pages and pages of “results” there will inevitably be something in that list that feels like the answer to the patient’s questions – because the test will spit out “answers” that cover every single condition and symptom out there. It’s easy to fall for the logical fallacy of thinking they’ve found their answer since it “fits”, and that’s what makes it so heartbreaking to watch.
These families spend money they don’t have, get false positive “results,” then go to their doctors who either don’t know enough about genetics and provide unjustified medical treatment based on a false diagnosis or they get turned away by genetics clinics and dismissed by doctors for having “junk” results –leading to a real breakdown in trust and rapport between patients and providers. I’ve seen this erosion of trust causing individuals to stop seeking medical care because no provider takes the time to explain why they’re being dismissive. The last thing rare disease families need are false promises by scam companies leading to medical distrust, which just prolongs being stuck in undiagnosed purgatory without answers or treatments. DTC companies are doing actual harm to rare disease patients and families who deserve to have their very valid medical concerns addressed by real providers who take the time to provide fact based information and actual guidance regarding the benefits and limitations of doing genetic testing.
“The last thing rare disease families need are false promises by scam companies leading to medical distrust, which just prolongs being stuck in undiagnosed purgatory without answers or treatments.”
Right now America is in a genetics crisis. Many genetic clinics, if you even have one in your state, have wait lists of 1-2 years, or longer. Many turn away common indications, such as hypermobile EDS, to try and shorten their wait times. Meanwhile, nearly 40% of individuals in the US report that they are not having needed medical care done due to financial barriers. So of course a test billed at “just a couple hundred” sounds tempting when each individual panel in a genetics lab is often at least $250 and whole exome/genome sequencing is (cash pay) upwards of $3,000 – 5,000. Some websites even offer free or $20-40 “reports” based on analyzing genetic “raw data” provided by other companies’ DTC tests, with the same poorly reviewed, inaccurate data dump, useless results. The bottom line is, these direct-to chaos tests are cheap because they are snake oil.
These pages of “results” also then leave individuals feeling like their real medical genetic testing is the “scam” as they only provide a single table of results, often between 1 and 5 variants. But the real value of the medical grade testing ordered by a trained specialist is their quality controls and their interpretation of the results. It takes skill to narrow genetic data down to only the top couple candidates for a possible answer. Anyone with a sequencer can spit out hundreds of garbage variants and call them the patient’s “answer” without any human oversight or skill. Anyone who creates a webpage can sell an “interpretation” of genetic data without any training or quality controls in place.
We need to not just talk about the harm these DTC companies are doing but also take action. By reaching out to alums from Harvard and Stanford I got two of these companies to stop advertising as “endorsed by them” without the institute’s signoff. I’ve gotten the CEO of one company removed from the national list of genetic counselors, as he is not a genetic counselor and was falsely advertising his company as a medical genetics service. I have personally reported these companies to the FDA and have had numerous patients who sadly wasted money on these companies also report them.
When you see harm happening to patients, you can and should speak up. Every little thing you do adds up to create real change.
We need to move past a whack-a-mole approach for every new falsely advertised snake oil option that appears but make real change to prevent them from preying on families who deserve so much better than these uselessly chaotic “results.”
“Rare disease families deserve answers. They deserve legitimate genetic testing options and access to genetic providers.”
I am outraged at these companies because as a rare disease patient myself, it truly breaks my heart to see people profiting over the stress, chaos, and misinformation sold to those who need our support and help the most. I have supported patients as they cried realizing they lost time, money, and hope to this nonsense. And I have cried myself after I’ve talked with these patients and families, as I wish I could step through that computer and hug my patient – or at least do something to stop the tidal wave of destruction these companies leave in their wake. Rare disease families deserve answers. They deserve legitimate genetic testing options and access to genetic providers. They deserve to be protected from DTC salespeople and to learn about genetic testing options from unbiased sources (not from employees of these DTC companies).It is not your fault if you believed the false advertising – they designed it to be misleading, but you and your patients deserve better.
In his poem American Sonnet Billy Collins compares a sonnet to “furrows in a small, carefully plowed field.” Classical sonnets are tidily structured works that more or less follow a format of 14 lines, often in rhyme, the last two of which offer a resolution to the problem or question set forth in the earlier lines.* The strictures and structure of a sonnet and the image of a plowed and furrowed field makes me think of how genetic counselors try to neatly organize genetic counseling sessions. The templated counseling notes we produce afterwards – some version of Patient Identification, Medical History, Family History, Counseling Provided, Summary and Recommendations – reinforce the idea of a structured session as well as the sonnet metaphor.
We try to impose structure, for reasons both good and not so good. In many clinical positions, most patients are coming to us with a handful of similar indications such that we wind up saying more or less the same things over and over, especially when we carry large patient loads. My roteness would become clear to me when a patient “interrupted” me with a question about something else altogether and I would forget where I was in my game plan. I was not listening to the message the patient was sending – they were not much interested in what I was talking about and they wanted to discuss something more important to them. Genetic counselors, with our professional insecurities, also subconsciously want to impress others with our arcane knowledge and prove that we can make an important contribution to the health and medical care of patients and their families. This manifests itself most acutely during the early stages of a career, when we are still slightly unsure of ourselves and are trying to establish a firm professional footing and reputation. But even wise veterans can get caught up in this style, including and particularly me (well, not anymore, now that I’ve converted to my favorite religion – Reitrementism).
While acknowledging the important role that numbers and information play in genetic counseling and patient care, a counseling session is at its core a psychological interaction between human beings. It took me – no kidding – a couple thousand counseling sessions before I even started to become a good genetic counselor and adapted my counseling to the basic psychological truth that the human mind usually expresses its emotional self in a non-linear manner. I knew this on a cognitive level but it took me years to actually incorporate this insight into my practice. To paraphrase Maya Angelou, people won’t remember what you said but they will never forget how you made them feel.
What does this mean in actual genetic counseling practice? I’m not advocating for omitting facts and figures or abandoning an over-arching loose structure. A counseling session should have a beginning and ending, and complex biomedical information often needs to be imparted. You can start out with a highly flexible plan of issues and information you think should be covered while at the same time be very willing to modify the plan or abandon it altogether to meet the unique needs of each patient. It might begin with a query as to what the patient wants to get out of the session, though some patients are better at articulating that than others and some just aren’t sure of what they want. But however you start, you need to be prepared for traveling with the patient as they veer off in often unclear directions that are sometimes different than what the patient originally articulated. Structure, numbers, information – they are so comforting and comfortable to us, like Collins’ neatly furrowed fields. But the safe zone of an organized educational format can make us hesitant to explore the unplowed fields of the patient’s psyche.
What we can discover in those unfurrowed fields is what is important to patients, why it is important, and how it influences the way patients makes sense of complex biomedical information and what they should do with it. Fear of going through treatment for cancer after having watched their parent’s body ravaged by chemotherapy. Anger at an employer for creating an emotionally or physically toxic workspace and attributing their cardiomyopathy to this environment. A deep belief in “natural cures” that is being challenged by their lack of efficacy in treating their child’s illness. Feelings of abandonment and resentment toward a parent who died when the patient was an adolescent and who is now a parent of an adolescent themselves. Fear of having a child with a disability. A marriage adrift on two different seas. Distrust of medical practitioners stemming from having been treated disrespectfully in past encounters. All of the technical information can be so damn scary they don’t want to talk about recurrence risks or the chances of getting cancer or variants of uncertain significance, at least not right away and not by listening to what sound like a verbal spreadsheet. Genetic counseling is supposed to make the patient feel emotionally safe, not the counselor.
What this requires is actually attending to what the patient is saying or asking, especially if it has little to do with what you are discussing. You don’t want to briefly comment on what sounds like a non-sequitur from the patient and then return to the safety of your comfortable structure. Following the patient’s lead can result in a session which travels in several different seemingly unconnected directions (Why is the patient going off at this angle?), loops back on itself several times (Hmm, why does the patient keep coming back to that?), or has you probing the patient with questions neither of you had anticipated (“And so you’re saying MRIs are scary to you because you have claustrophobia and you’ve also read that the MRI’s magnetic field is thousands of times stronger than the earth’s magnetic field at its surface, and that’s why you are reluctant to undergo hereditary cancer testing?”). It can become a near stream of consciousness session that resembles James Joyce’s Ulysses more than Elizabeth Barrett Browning’s tenderly romantic How Do I Love Thee?. Joyce’s novel begins with the famous opening line that seems to presage a typical narrative – “Stately, plump Buck Mulligan came from the stairhead, bearing a bowl of lather on which a mirror and a razor lay crossed.” – then quickly changes tone and explores the depths of the minds of the novel’s characters and ends with Molly Bloom pouring out her innermost thoughts in an unpunctuated iambic-pentameter-be-damned eight sentence ~22,000 word uninhibited and unfiltered soliloquy. Kinda’ like a counseling session can go (Nothing against Barrett Browning. She is a marvelous poet; just a different style than Joyce’s).
I don’t know how AI chatbots will play out in the genetic counseling arena and how they might influence the structure of genetic counseling sessions. It seems possible that they might one day be capable of carrying out a psychologically sophisticated interaction with a patient that matches a counselor’s skill set as well as taking into account the patient’s socioeconomic situation, though I suspect not in the immediate future and hopefully not until the ethical issues have been addressed (for an amusing take on chatbots and genetic counselors, check out my post Genetic Counselor Reinvented). My bigger immediate concern is that administrators will simply see chatbots as a replacement for genetic counselors rather than as an ancillary tool for genetic counseling. Or that administrators will employ a strategy that employs both genetic counselors and chatbots but increases counselors’ patient loads on the premises that chatbots are doing a lot of the work and so you can fit more sessions into a counselor’s schedule. This ignores the emotional toll on genetic counselors who work with patients in stressful situations and will likely lead to counselor burnout and poorer quality patient care.
The potential and concerns about AI aside for now, the semi-chaotic session is often more valuable to patients than the biomedical lecture. Yeah, it can look and sound like a mess and be just as dense and difficult to understand as Ulysses. But that mess is where the beauty of the patient’s mind lies. Which is why we need to use our counseling skills to sort through the mess and understand the psychological meaning of the patient’s words, beliefs, actions, and choices. Hence the wonderful messiness of genetic counseling.
The Brain — is wider than the Sky — For — put them side by side — The one the other will contain With ease — and You — beside — by Emily Dickinson
Over the centuries, poets have played with the format of the sonnet to breathe new life into it, such as Wanda Coleman’s American Sonnet 91 and other of her decidedly non-linear poems that explore race and racism in America.
Polygenic risk scores* are all the rage these days. Thousands of articles and research studies have attempted to link polygenic scores to just about every medical condition, behavior, and trait you can think of, and a few I had not thought of such as reproductive behavior. They have contributed to improving our understanding of human genetic architecture, hold potential for guiding treatment decisions, and have started to open the black box of gene-environment interplay, to name a few applications. Polygenic scores have laid bare the racial/ethnic bias in genetic data bases that have proven to be overwhelmingly comprised of people of Northern and Western European ancestry and shamed the genetics community into striving to better serve all communities. They have also been used inappropriately in clinical practice, such as with preimplantation genetic testing to predict potential height and intelligence of an embryo (quite poorly as it turns out) to determine its “implant-worthiness.”
The value of polygenic scores in clinical settings, despite the optimism expressed in many of the publications, remains unproven for the most part. Time and more research will presumably filter out the clinical winners from the losers. But we also need to sort through the thorny ethical, economic, and social justice issues with equal intensity and resources.
One particular application of polygenic screening is undermined by a naïve understanding of human psychology and a failure to learn from past experience in genetics – population polygenic screening for common conditions such as cardiovascular disease, diabetes, hypertension, and cancer. I don’t believe that polygenic scores will have a particularly strong impact on reducing the impact on morbidity and mortality from these common conditions. There is ample evidence that genetic testing has little or no effect on risk-reducing behaviors. In fact, I’d go as far to say that the research investment into population polygenic screening for these conditions is disproportional to their likely medical benefit.
The aim of polygenic screening for health conditions is to produce a number, some likelihood that a healthy person will eventually develop condition X, and that risk estimate would be the basis of medical recommendations to reduce or manage the risk. As with all likelihood estimates in clinical care, polygenic screens, with or without inclusion of demographic and clinical variables, will be imperfect, maybe slightly more or less imperfect than estimates derived by other means. Genetic counselors have been dealing with such numbers since we first entered clinics half a century ago and began providing patients with empirical recurrence risks for genetic conditions or the probability of having a baby with an aneuploidy based on parental age or screening results. Some think that providing numbers is the purpose of genetic counseling but it turns out to be only the beginning of the counseling session (emphasis on counseling).
The naïve assumption underlying polygenic screening for common conditions is that the risk number will magically motivate people to undergo more frequent colonoscopies, breast MRI, change their diet, stop smoking, exercise more, and reduce the stress in their lives. Yeah, well, good luck with that, at least on any large scale, on a sustained basis, and outside the context of a research study of self-selected participants conducted over a short time span. Sure, some people will be nudged into screening uptake or lifestyle changes, and a smaller percentage may even keep it up. But decades of experience have shown that most people are going to continue doing what they are doing with their lives – healthy behaviors or not – thank you very much.
There is a persistent but mistaken view in genetics, and medicine in general, that the human psyche is an objective statistical risk calculator and the “right” number will motivate people to do the “right” thing. This is a zombie concept that, like nondirectiveness, refuses to die. But the human mind is a complex and not entirely rational system, at least not like a Sherlock Holmes ratiocinative detective type of rationality. Numbers are embedded in a patient’s psychological, emotional, life-history, social, economic and political matrix that can vary over the short and long term. Numbers are interpreted or misinterpreted or denied or ignored such that it fits into the patient’s elastic view of the world. The results are often decisions that seem to make no sense or appear ludicrous to medical professionals but makes perfect sense to patients at this point in their lives. That decision could change over time, sometimes for apparent reasons such as the death of a family member, and sometimes for no obvious reason. They can even change from a “good” decision to a “bad” decision.
Of course, some people seem to be nominally objective decision-makers, the so-called engineer or statistician types. The patients who suddenly become actively engaged in the genetic counseling session once numbers are tossed out for discussion, dissecting and closely questioning their accuracy, how they were derived, and what the confidence intervals are. If you bring up statistical measures such as area under the curve or Cox proportional hazards, they even seem mildly sexually aroused. But the engineers and statisticians ultimately interpret numbers psychologically, just like the rest of us.
I don’t mean to imply that polygenic scores are totally useless. One of our jobs in medicine is to find ways to reduce the impact of disease on patients’ lives and polygenic scores might provide some help to that end. Research into polygenic traits can contribute to the scientific understanding of human and medical genetics. And polygenic scores will likely have some clinical utility. I can see some settings where a health risk has already been identified and a polygenic score can help further refine that risk. For example, polygenic scores might modify the ovarian or breast cancer risk or the age of onset in a patient who carries a pathogenic BRCA1 variant. It could then influence timing of risk-reducing surgeries or help determine if such surgeries are even necessary. Readers can undoubtedly think of other scenarios where polygenic screens might help influence decision making by high risk or affected patients.
We need to scale back expectations that population polygenic screening will significantly reduce the morbidity and mortality stemming from common conditions. I suspect that its impact on disease and death will be modest and at times unclear, perhaps with an occasional success story. The minimal research that has been done to date on the uptake of screening or other medical recommendations after a polygenic screen have produced mixed results and are not overwhelmingly convincing, though of course further research may prove otherwise.
There are also technical reasons to suspect that polygenic screens may not work well on a population level as measured by detection rates, false positive rates, and positive predictive values. In addition, existing inequities in access to and utilization of health care will further reduce the utilization of polygenic scores and subsequent follow-up of medical management recommendations by patients. If you don’t have access to good medical care and the appropriate interventions, or you can’t pay for it, or you have a lack of trust in the system, what good is screening?
Figure 2 from Hingorani AD, et al, BMJ Medicine 2023;2:e000554. doi: 10.1136/bmjmed-2023-000554Performance in screening estimated for polygenic risk scores included in the Polygenic Score Catalog from April 2022. Limits of each box represent interquartile range and horizontal line within each box is estimated detection rate for a 5% false positive rate (DR5) based on performance metrics reported for corresponding polygenic risk scores. Selected diseases are colour coded into categories cancers, cardiometabolic conditions, ocular diseases, allergic or autoimmune diseases, bone disease, and neuropsychiatric diseases. Horizontal line is estimated median DR5 value based on performance metrics for all 926 polygenic risk scores and all diseases studied in the Polygenic Score Catalog.
We need to take a hard look at just what we expect to achieve with polygenic scores. A lot of energy, resources, and finances go into research and publications about polygenic screens. Perhaps that time and money could better be directed to research where benefits of polygenic testing are more likely to be realized or to other areas of genetic research altogether, like how and why people make decisions about healthcare and how it is affected by personal, economic, social, historical, and political factors (think Covid vaccination uptake).
The medical genetics community may be resistant to my recommendations. Some of that resistance will be based on thoughtful and understandable disagreement with my opinions and their own assessment of the potential of polygenic scores in a population setting. But underlying some of that disagreement, and some of the enthusiasm for polygenic scores, is that all the players in the genetic testing game have blind spots and conflicts of interest. Researchers in the academic/clinical research industrial complex need grants and publications to further their careers. This includes not only Principal Investigators, but also the many other people necessary to conduct research – ethicists, research assistants, junior investigators, etc. The genetic counseling profession has for better and worse taken up genetic testing as its defining role in the medical system, and genetic counselors working in direct patient care demonstrate their economic worth to their employers by increasing the downstream revenue that results from genetic testing (revenue raised directly by genetic counseling alone is rarely enough to cover salaries and benefits). Commercial laboratories make their money by selling genetic tests; not a bad thing in and of itself but it can cloud one’s views. With all these players all talking the same game, they can lose sight of what’s good for the fans and unintentionally prioritize what’s good for the teams, such as citing improving institutional revenue from increased imaging as one of the benefits of polygenic scores or direct-to-consumer commercial labs offering polygenic scores when the health benefits remain at best unclear. I am not suggesting that researchers, genetic counselors, and labs are unethical and I am not questioning their dedication to quality medical care for patients. They are just being human and the human mind has a way of persuading itself that it’s doing the noble thing when in fact it may be putting its own interests first.
People interpret numbers how they want to interpret them. We see evidence of this on a large scale every day. Climate change is ignored in the face of rising temperatures and melting ice packs. Election results are denied because they don’t conform to the desired outcome. Millions of pandemic deaths are explained away as falsified or manipulated numbers to justify disregarding public health measures. This holds equally true for the results of genetic testing in populations. If we want genetic testing to be useful to our very human patients, we must develop a more sophisticated and less naïve understanding of the human psyche.
* – There is some controversy about the name “polygenic risk score.” “Risk” tends to evoke anxiety in our minds; typically, one is not at risk for good outcomes, like winning a large lottery prize. It also implies a value judgment on the condition being screened for. Many people would argue that deafness or autism are desirable or normal outcomes, not something that one is at risk for. Alternatives include “polygenic score” or “polygenic index.” I like my own coinage – “polygenic screen” – when referring specifically to polygenic risk scores for medical conditions in healthy people since it implies the test is not diagnostic (yes, I know, people tend to confuse diagnostic tests with screening tests à la NIPT). In this posting, I use all these terms more or less interchangeably because, well, I can’t make up my mind which I prefer.
In order to distinguish between the various applications of polygenic scores, consider these suggestions for a possible terminology:
Polygenic Index – when used to predict a non-medical trait, such as height or intelligence.
Polygenic Screen – when applied to population screening for common medical conditions.
Polygenic Risk Score – when applied to a population previously identified as being at high risk for, or affected by, a medical condition, such as breast cancer, to potentially guide treatment, risk reduction, and surveillance recommendations.
To distinguish between a polygenic only model and a model that combines SNP analysis with clinical and demographic factors, a “+” could be added, e.g., Polygenic Screen+– Breast Cancer to denote a breast cancer risk prediction model that incorporates SNP analysis with the Tyrer-Cuzick or other breast cancer risk prediction model.
The collective memory of eugenics is that it was an ideology of archconservatives that thrived during the first half of the 20th century and whose demise was hastened by the horrors of Nazi Germany. We like to think that we now know better. Better science, better morals, better guiding ethical principles. Heck, we must even be better people. It may be a comforting story, but historians of science have been pointing out for decades that this collective memory is flawed. Eugenic ideologies and policies, usually under different labels and in various forms, can be found today in science, medicine, and social policies.
Strands of eugenic beliefs also became embedded into popular culture. For example, as historian of science Paul Lombardo has demonstrated, references to eugenics could be found in the advertisements of popular magazines and newspapers in the first half of the 20th century, suggesting that the average American was familiar enough with eugenics that the term needed no explanation. For marketing purposes, eugenics implied excellent consumer products such as diamonds, hair styles, and hair shoes, in much the same way that many companies today will state that the quality of its products or the company’s dedication to customer service is part of the company’s DNA. There are many other examples of eugenic themes in 20th and 21st century novels, films, comics, and video games.
Along these lines, I recently came across two Walt Disney cartoons that echo eugenic themes. I couldn’t believe it at first. I thought maybe it was just my hyperactive eugenics paranoia kicking in and deluding me. After all, I tend to see eugenic monsters lurking under my bed at night. But the more I studied the cartoons, the more convinced I became.
Disclaimer: I have no reason to believe that Walt Disney himself was a dyed-in-the-wool eugenicist or that the Walt Disney Company is a front for a nefarious eugenics media empire. Rather, these cartoons illustrate how eugenic ideology was so pervasive that it subtly and not so subtly became woven into the fabric of American popular culture. It could appear in a cartoon without the creators having a single eugenic bone in their body. Or it could manifest under a different name, so disguised that a cartoonist might not recognize it for what it was.
The first cartoon, Goofy’s Adventure Story from 1954, tells the story of the family history of the Disney character Goofy. Goofy is an anthropomorphized dog who first appeared in 1932 – the heyday of classic eugenics – as the character Dippy Dawg. The cartoon includes a family tree in reverse order of tree growth, i.e., with the ancestral Caveman Goofy at its apex and 1950s Goofy at its base (which, curiously, is how family trees were typically drawn until about the 15th century). Descending between the two is a lineage of historical Goofy characters. Each ancestor is basically a stereotypical White European (for the moment, ignoring Goofy’s canine heritage*). In the cartoon, each character does something, well, goofy, in keeping with the character’s namesake trait. Goofy appears to be part of a patrilineal society since there are no female ancestors on the tree.
The family tree was a powerful symbol for eugenicists, who recognized the value of graphics in getting their point across. The many pedigrees of “feeble-minded” families produced by eugenicists were used to “prove” that intelligence was inherited in Mendelian fashion and that the people at the lower end of the intelligence spectrum were breeding at such incredible rates that the very existence of society was threatened by their reproductive drive, low intelligence, and propensity to crime and poverty. The pedigrees of “feeble-minded” families – typically poor and from “degenerate races” – reflected the race and class biases of eugenicists, who were primarily economically well-off Northern and Western White men.
Goofy’s family tree is a variation on these eugenic pedigrees. Goofy’s tree is peopled with Noble White Man tropes so beloved by eugenicists, such as Roman emperors, Greek warriors, knights in armor, and Pilgrims. In keeping with Goofy’s nature, these figures are presented in comic form. But the comic form gets at the essence of the connection to eugenics. Think about it for a moment – the name Goofy is synonymous with “feeble-minded,” a connection reinforced by his signature “Hyuk, Hyuk” laugh and two widely-separated upper teeth (which don’t look like canines to see). Disney, of course, wasn’t trying to revive classic eugenics. Rather, Goofy’s pedigree illustrates how the eugenic notion that intelligence was inherited and ran for generations within families was so engrained into the public consciousness that, even without thinking about eugenics. it was natural to create a “feeble-minded” cartoon character who has a family tree full of “feeble-mindedness.” Goofy’s family history is a modified and cartoonized version of the pedigrees of the Jukes, the Kallikaks, the Hill Folk, the Mongrel Virginians, the Pineys, the Nam Family, and the many other “degenerate” families described by eugenicists.
A rendering of the Kallikak Family tree from a 1950s psychology text (contemporaneous with Goofy’s family tree), based on the 1912 book “The Kallikak Family: A Study in the Heredity of Feeblemindedness” by Henry Goddard.https://en.wikipedia.org/wiki/The_Kallikak_Family
The Goofy family tree also includes an odd appendage, one that I have decided to believe is unintentionally inappropriate and reflective of what was considered acceptable at the time rather than a, uh, racist dog whistle. Dangling from the lowest branch on the left is a noose. I am not exactly sure what a noose is doing here although I guess it’s somehow connected to Wyatt Earp Goofy, who appears to be nailing a Wanted poster to a tree. Not that I expect a cartoon to be historically accurate, but Earp is not particularly associated with hangings, and in fact helped disperse a mob that was intent on hanging a man accused of murder. The noose, of course, is an image used by White supremacist racists to try to strike fear in the hearts of Black people in America. Along these lines, in the cartoon Wild Bill Goofy shoots a Native American in a manner that’s somehow supposed to be humorous, and the appearances of Native Americans and South Seas “cannibals” are depicted stereotypically.
In another weird twist, the country the Goofy Family Tree appeared on a postal stamp issued by Uganda in 1992, celebrating the 60th anniversary of the creation of the Goofy character (Disney characters were licensed for use on postage stamps in many countries).
In the other eugenic-themed Disney cartoon, titled Family Planning, Donald Duck helps a disembodied narrator explain family planning. The cartoon does not detail the specific methods of family planning other than “taking pills” and “using simple devices.” Just as well, I guess. I for one was not interested in Donald Duck demonstrating how to use a condom or Donald and Daisy practicing the rhythm method.
Some of the Population Council’s early presidents had strong ties to pre-World War II eugenics, most notably Frederick Osborn. Osborn helped create the journal Eugenics Quarterly, was a founding member of the American Eugenics Society and a member of Britain’s Eugenics Society, and once characterized Nazi eugenics as “an important experiment.” After WWII, he apparently had a fall-off-his-ass experience and began portraying himself as a severe critic of classic eugenicists such as his uncle Henry Fairfield Osborn. He shifted his focus to positive eugenics (i.e., encouraging the “right” people to breed and encouraging the “wrong” people to voluntarily curb reproduction) and acknowledged the role that environment played in an individual’s development and lot in life, what might euphemistically be called a kindler, gentler eugenics.
Despite Osborn’s claim to the contrary, these two quotes from 1965 and 1963, respectively, demonstrate that he had not fully shed some of his hard core eugenic beliefs:
…the average genetic character of parents of unwanted children is likely in the long run to be below average. An unusual proportion of these unwanted children grow up to be juvenile delinquents, unemployed, or social charges.
Every racial group has a certain proportion of genes for high ability…. It appears that ever since World War II, Negroes as a group have been increasing in numbers more rapidly than the Whites, with a probable trend during this period towards producing relatively fewer able individuals. This is the kind of dysgenic situation which eugenics aims to ready.
Osborn was no longer president when the cartoon was produced and as far as I know did not play a role in developing it. But his eugenic philosophy strongly influenced the organization’s policies during the 1960s. It’s this Osbornian view of humanity that guides the message of the Disney cartoon.
The cartoon’s central character is a peasant farmer with a skin tone a shade or two darker than white and who speaks English with what sounds to me like a Central American accent. When the family has only 3 children, the farmer is able to provide for his family – enough food, schooling, and a few simple possessions such as a radio. But, according to the cartoon, if the family goes on to have 4 more children, the farmer will no longer be able to provide enough food or otherwise meet the basic needs of his family. The parents become so tired they can barely care for their children, who grow weak and sickly. When the sons grow up, the small family plot will have to be divided among them, restricting their ability to care for their families. Heaven forbid, should the family move to the city they will be even worse off because they can’t afford to live there. The narrator’s solution is for the peasant to practice family planning so that reproduction is not “left to chance” and “you can only have the children you want.”
Eugenic themes were not confined to cartoons. They can be found in other areas of popular culture from that era and even up to today. The Beverly Hillbillies (“a poor mountaineer who barely kept his family fed”) are the cultural descendants of Charles Davenport’s Hill Folk. As are the inhabitants of the hills of northern Georgia in James Dickey’s novel Deliverance (“Nobody worth a damn could ever came from this place.”) who terrorized the rich urban men seeking to display their manhood by spending a weekend rafting a wild river. Or, from a previous generation, the immigrant-hating horror novelist H.P. Lovecraft who wrote of unimaginable alien horrors lurking in the hills of New England (“West of Arkham the hills rise wild… When I went into the hills they told me the place was evil.”). In a clever thematic manipulation, the current TV series Lovecraft Country features Black characters facing the monsters of White racism across America’s 1950s South.
The current spate of zombie movies, novels, and television shows can be read as eugenic, with their mutated throngs of human monsters threatening the existence of Western civilization. Perhaps it’s no coincidence that the popularity of the zombie genre is blossoming during a time of anti-immigrant sentiment in Europe, America, and other places. Eugenics has an uncanny ability to morph and adapt to different times and different cultural milieus. And, like zombies, it refuses to die.
– Someone really should perform whole genome sequencing on Goofy and Pluto to finally resolve the long-standing debate about the differences between the two, Goofy being a canine who is bipedal, language fluent, and a friend of Mickey Mouse whereas Pluto is a quadrupedal canine, incapable of speaking, and is Mickey’s pet. Surely the difference lies in their genomes.













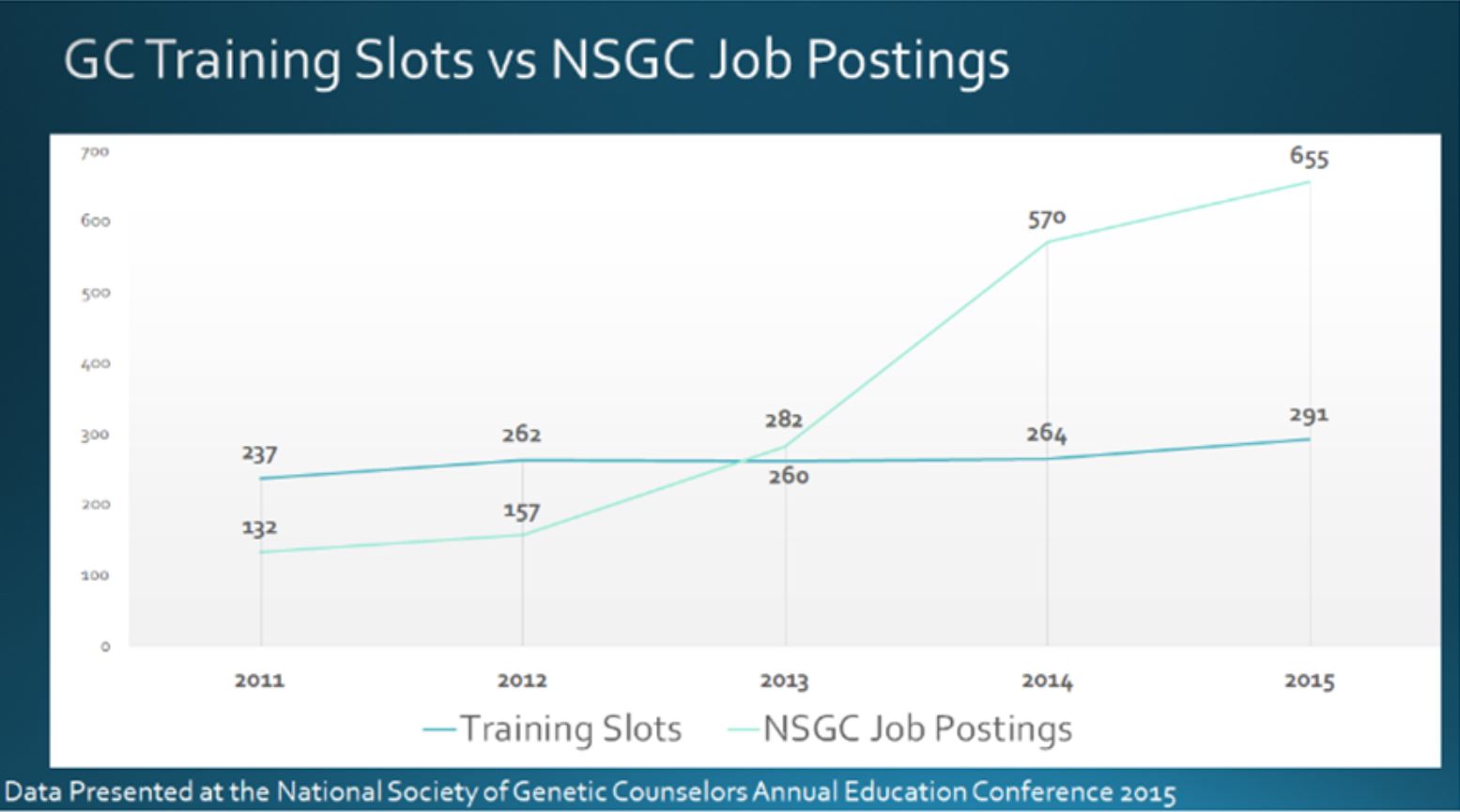







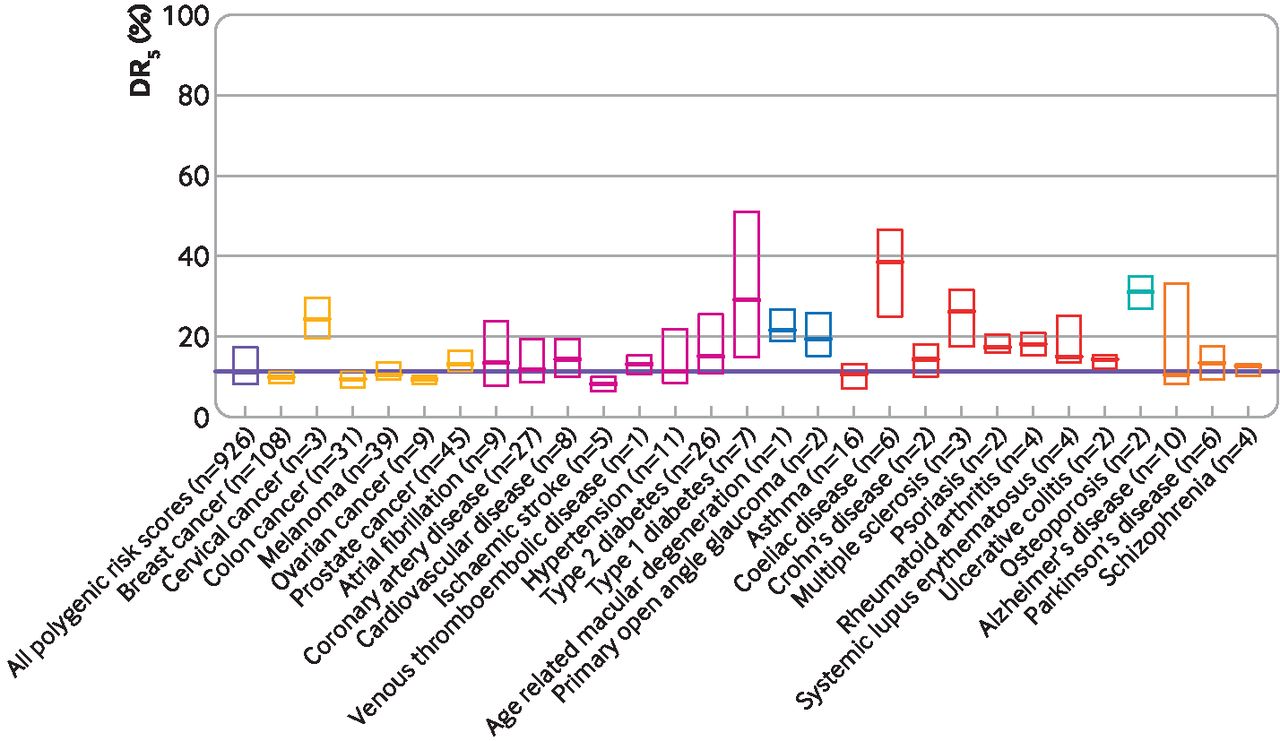


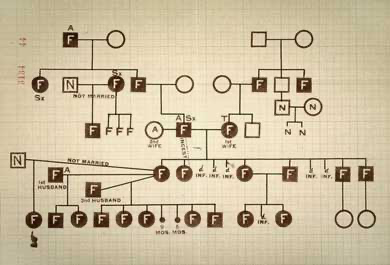



{kind=link}
{kind=link}