Let me start by saying that I am not sure yet about what genetic counselors should be doing to fight the racist, vile, despicable, UnChristian/unMuslim/unJewish/unEvery Other Religion-In-The-World policies, actions, and statements of the Trump administration. I do know that we should not be cowering quietly in the corner, overwhelmed by the crap coming out of the bowels of (F)Elon Musk and PINO Trump (President In Name Only) in peristaltic waves. I have been thinking about this for a while and don’t have any really good answers, other than praying for debilitating strokes for those at the top (?bottom?). But I offer some thoughts and suggestions here. Some may be useless or impractical or simply not do-able.
In no particular order, consider these ideas, big and small, both on an individual level and on an organizational level:
Download the 5 Calls app. The group behind this app “research[es] issues, write scripts that clearly articulate a progressive position, figure out the most influential decision-makers, and collect phone numbers for their offices. All you have to do is call.” It provides phone numbers of senators and representatives along with a script about specific topics to read when you leave a voice mail. Calling is probably the most effective way to communicate with your government representatives, more so than letters, postcards, and emails.
Offer individual safe spaces – in person, phone, email, zoom, whatever – for colleagues to confidentially share their anxieties, fears, anger, and other emotions. Sometimes you just need to decompress, so, when appropriate, share comfort food and wine/whisky/beer/cannabis (where legal).
Encourage our professional organizations (NSGC, ASHG, ACMG, and whatever other organizations you belong to) to take a principled stand and boldly and clearly reaffirm their commitment to diversity, equity, and inclusion. Yes, it’s only a statement, and those may not add up to a hill of beans, but at least membership knows where their organizations stand, and offers something concrete to hold them accountable for.
Our professional organizations have lobbyists. Can their services be utilized to lobby representatives?
Our organizations also employ lawyers. Can they guide NSGC et al. to sign on as plaintiffs in relevant law suits against the government, where they might have some legal standing to file, such as those that might involve NIH funding or care of transgender patients? Or at least file amicus briefs?
Can NSGC et al. provide safe spaces, something as simple as zoom chats or webinars, where members simply get the opportunity to share their fears and anxieties, and keep us directly up to date on what actions they are taking? Can participants be anonymized if they so choose, if they are worried about their personal safety?
Have our organizations adopt as their temporary motto in bold capitals on their websites “Fuck Trump and Musk”? Okay, well, maybe that’s a bridge too far. But it would be really cool.
Take to the streets in peaceful massive protests. I do not condone violence of any sort, other than in self-defense. This may involve risking your personal safety, as some Pro-Trumpers now assume they have the clearance to bust a few heads, free from legal sanction. And one could easily imagine the federal government pressuring local law enforcement to deal severely with protesters.
Run for local offices – school boards, town/city councils, whatever – to formulate and fight for respectful, democratic, and decency-affirming policies.
Volunteer for organizations that work to do good in the world.
Write blogposts, letters to the editor, editorials, whatever media, decrying the inhumanity and ignorance of the government’s actions. Use your genetic counseling communication skills that we are alw
Don’t let the bastards get the best of you. Fight’em tooth and nail. Proudly wear our Woke buttons (“I’m Woke – Are You Asleep?”).
If it is financially feasible, donate to organizations that are fighting the good fight.
Event though we don our costumes and capes at work and play Super Heroes fighting for our patients, and even though there are some Marvel Universe villains running the governmental show, remember that each and every one of us is just a human being. Don’t take the weight of the world on your shoulders alone, and don’t emotionally whip yourself if you feel overwhelmed or temporarily defeated. Even The Incredible Hulk has a human core.
I encourage readers to suggest more. We need to do this for ourselves, our colleagues, our patients, and our country. Those genetic counselors who feel vulnerable in their lives and jobs are given a pass here. It’s up to the rest of us to take care of all of us.
Back on January 20th, American democracy and decency began to swalllow a poison pill of its own electoral making. The fallout has been all kinds of horrible, nationally and internationally, except in Moscow where Putin is having a belly laugh because America is doing his dirty work by destroying itself. The US Constitution is being shredded. People who are transgender, gay, non-White, and all the other non-majority varieties of American demographics feel that their very lives are threatened. The employment of every “DEI hire” (racist code word for Black) is on the chopping block. Many of our patients may lose access to health care through Medicaid funding cuts, fear of being deported, or prohibitions of basic medical care for transgender people. We are looking at the potential destruction of the NIH, one of the world’s great research institutions. Genetic counselors employed by the federal government or on government grants may either lose their jobs or be forced to work in an ethically intolerable environment. The terrifying list goes on and on. The over-arching hateful personal message of these policies is “If you ain’t cis-hetero-White, you ain’t right.”
I have nothing original to add to what has already been better said by others about these matters.* Here I want to focus on the implications of the Updated NSGC Guidelines on Pedigree Nomenclature for the passage of the Access To Genetic Counselor Services Act (I am one of the authors of those pedigree guidelines, and incidentally, a minor revision of some of the Tables will soon be published). A small matter in the great scheme of things, but of particular salience to the future of the genetic counseling profession. The financial survival of clinical genetic counselors in the US hinges on being recognized as Medicare providers. This effort has been ongoing for some 20 frustrating years or so but over the last few years we’ve started getting closer to success, fingers crossed.
So why should the new pedigree nomenclature crash those hopes? After all, they are just a bunch of geometric shapes. But we have given meaning to those shapes, meaning which directly clashes with the Executive Edict, er, I mean Order “DEFENDING WOMEN FROM GENDER IDEOLOGY EXTREMISM AND RESTORING BIOLOGICAL TRUTH TO THE FEDERAL GOVERNMENT,” that, based on ignorance and hate, defines sex as follows: “(d) “Female” means a person belonging, at conception, to the sex that produces the large reproductive cell. “Male” means a person belonging, at conception, to the sex that produces the small reproductive cell.” Well, I guess that those of us who were lucky enough to be born with “reproductive cells” are going to have to line up and start getting those reproductive cells measured and compared. I wonder which cells they are going to measure – Sertoli cells? Leydig cells? Spermatids? Uterine cells? Luminal epithelial cells of the uterus? Ovarian thecal cells? All are necessary for reproduction, and all of different sizes. Of course, at conception, no one has any of those cells so I have no idea what these criteria mean. And sex can be categorized by chromosomes, genes, anatomy, or hormonal profiles, all biologically plausible criteria but not uncommonly incongruent.
The head of the US government has made it clear that any definition of sex that, uhh, deviates from this definition is the product of “Woke” ideology and DEI policies (I really don’t know what constitutes Woke ideology – compassion? decency? the teachings of Christ? – but I reckon it’s better than Sleepy ideology). Anyone or any organization that supports Woke ideology is an enemy of the state and will not be tolerated. The pedigree nomenclature, by emphasizing the importance of gender and the subtle shadings of biological sex, is diametrically opposed to US government policy. All the more reason to support the nomenclature, I say.
But what happens if the Access to Genetic Counselor Services Act actually comes up for a vote before Congress? Well, perhaps the most publicly available product of the genetic counseling profession is the pedigree nomenclature. Sure, within the NSGC itself, there are all kinds of policies and initiatives that support DEI, programs that have been met with varying degrees of success and frustration. By and large those are internal, and not openly available to non-members. But as an Open Access article, the pedigree nomenclature is widely available to anyone with Internet access and the nomenclature is the standard for most genetics journals, not just the Journal of Genetic Counseling. More tellingly, the simplicity of those symbols that allows them to effectively communicate complex information also allows them to clearly communicate just how much they contravene the Trumpian concepts of sex and gender, even to someone who has minimal grasp of human biology. I can imagine an NSGC President testifying before Congress about the bill and being asked “So, Current NSGC President, in your organization’s sanctioned pedigree guidelines, I see squares and circles and common sense tells me that those are males and females, respectively. Can you tell me what this diamond symbol is? And what are those funny abbreviations like AFAB mean beneath some of the symbols? Are genetic counselors using geometric symbols to secretly support Woke DEI propaganda? The US government does not support an organization that does not preach biological truth!”
I am not saying that we should publicly reject or downplay the Pedigree Nomenclature Guidelines or NSGC’s DEIJ initiatives. To do so would be an act of moral cowardice, a betrayal of our colleagues and patients, and just plain wrong. We need to fight like hell for them, even if we have to pay a steep professional price. There are more important things in life than Medicare coverage.
Should I stay or should I go now? If I go there will be trouble And if I stay it will be double – From The Clash’s “Should I Stay or Should I Go?“
Working with patients as they make decisions is one of the core components of genetic counseling. It’s not the only thing genetic counselors do, but we sure do it a lot. Some of these decisions are relatively minor while others can be life-changing, irreversible, and have life and death implications. When the decision does not call for an immediate choice, the patient has some breathing room to weigh the situation and work through the cognitive and psychological issues. In other circumstances, there is the added complication of a time-critical decision that must be made within days or hours. But either way, no matter how much we educate, engage, reciprocally engage, or center the patient, making decisions can be gut-wrenchingly difficult.
All genetic counselors have dealt with this in some way. Should I have a cfDNA prenatal screen? Just for aneuploidy or include some of the microdeletions too? If it’s positive, should I have an amnio? I really want that germline breast cancer panel but those results can be awfully scary, or maybe worse, ambiguous. Should I have a unilateral or bilateral mastectomy? Should I subject my child to a new but unproven treatment for a genetic condition when that treatment may have serious side effects and may not even be effective? Should I let my asymptomatic child who carries a low penetrant pathogenic variant for a hereditary cardiomyopathy participate in high intensity sports like crew or kayaking so they can have as normal a childhood as possible?
The genetic counseling literature often talks about informed choices. But after about the first genetic counseling session in your career, you quickly realize that choices involve a lot more than just informing. Complex emotional and psychological matters come in to play as patients process the information and try to figure out what the different options might mean for them, their families, their emotional states, their finances, and their psychological adaptation to their post-decision lives. It’s not simply a matter of weighing pros and cons. It’s more like trying to piece together a jigsaw puzzle when you don’t have a box cover to tell you what the completed puzzle should look like and you only have a limited time to do it in. How do all these damned pieces fit together to create a coherent picture?
The hardest part is that patients just about never know if a decision is good or bad until after they’ve made it. Sure, sometimes (maybe most of the time? I don’t know), decisions turn out to be the “right” one. But there is no way that patients or genetic counselors can predict the future and reassure one another that the particular patient choice will turn out to be for the best, or at least not for the worst. There are just too many unknowns and unknowables. We think we know ourselves but then we are faced with a new reality and suddenly we don’t know ourselves so well. I didn’t think that early menopause would be this bad. I believed I could terminate a pregnancy if I thought the baby had a profoundly serious condition, but now that I know it, I’m not so sure I can go through with a termination. After having watched our mother die of ovarian cancer and supporting me through my breast cancer treatment and decision about having genetic testing, I was sure my two sisters would be relieved to have the genetic information so they could learn their own risks and act accordingly to reduce their risks. Instead they have gone into a psychological tailspin and one of them isn’t even talking to me anymore.
Then there is the matter of people and their values changing over time. This can alter perspectives on whether a decision made years ago was for the best. For example, a patient might have been an atheist but as they’ve gotten older, they’ve found great comfort in Christianity or Islam or whatever faith and now their views are guided by religious beliefs. Or conversely, deeply religious people may lose their faith after witnessing so much cruelty and senseless suffering in the world. A 30 year old may have been dead set against having children and decided to undergo sapling-oophorectomy to reduce their cancer risks but afterwards has a change of heart and regrets having lost the ability to become pregnant. Someone may have been a staunch supporter of abortion for themselves and others but their personal ethics and philosophy have changed over time and they are wracked with guilt because they now feel that abortion is morally wrong.
Unpredictable externalities may also influence how people come to view their decisions over time. Someone might choose an expensive but unproven lifelong treatment for themselves or their children but then lose their job and their health insurance, leading to deep medical debt and perhaps loss of housing, and to top it off, the medical condition has only worsened over time. Someone reluctantly undergoes genetic testing for Huntington disease to establish the risks for their two siblings, and though the patient thinks it was a bad emotional decision for personal reasons, they take comfort in learning that their siblings do not carry the pathogenic triplet repeat expansion. Shortly thereafter, both siblings die in a pandemic after having refused a vaccination. A woman undergoes a risk-reducing saplingo-oophorectomy but winds up with serious and life-threatening post-operative complications.
I’m not trying to push the pessimitic and unhelpful message to patients that they should just give up and flip a coin or turn to a tarot reading because it is impossible to make good decisions. Instead, we need to help them understand that often there may not be a clear-cut best choice at the time they are making the decision. And genetic counselors should feel free to constructively criticize and explore a patient’s choice if it shows they clearly did not understand the underlying technical information or it does not seem to align with their values, while doing our best to filter our our own biases and counter-transference issues. Patients need to recognize that over time they may change their view of whether their decision was the right one or the wrong one or some mix of the two. They don’t have too much control over the future. But we can help them understand that they have done everything they could to make the best possible decision at that time They are decent, compassionate human beings who are just trying to do the best they can in a very complicated world.
Beyond the genetic counseling sphere, the difficulties of decision making arise in all of our everyday lives. Should I take this job or that job? Is this the best person to hire for the job (I swear that, despite all the interviews and glowing letters of recommendation, you never know what somebody is like as a co-worker until you’ve worked with them)? Should I buy this house or that house? Is this the person I want to marry? Are we at the point where divorce is the best option? Should I attend college or learn a trade and become a plumber or an electrician? Should I stay at home to raise my children or continue working and somehow manage to pay for child care? We can’t know the answers to these questions. We can only do our best and not kick ourselves when life doesn’t turn out as we thought it might.
I am in the midst of watching the Jeux olympiques d’été de 2024 (aka The Paris Olympics, the XXXIII Olympiad), one of the benefits of retirement. As I write this, Rowdy Gaines is narrating a swimming event with his usual infectious and unconstrained enthusiasm (every country has its own Rowdy Gaines equivalent for various sports). Watching the marvelous bodies and performances of these athletes triggered some thoughts about which bodies are or are not allowed to compete. More specifically, I began reflecting on the history of using genetic testing to determine which athletes would be permitted to compete in women’s Olympic sporting events. It’s a tale of how the inappropriate use of genetic testing can have far reaching ethical, political, legal, social justice, sexual bias, and racial bias effects.
There is wide agreement that elite biological male athletes generally have superior physical performances compared to elite biological female athletes in some sports. It is an understatement to say that evaluating athletes to determine if they are “female enough” to compete as women is highly controversial, including among athletes themselves. I am not going to enter that fray here. The problem is that biological sex is more of a spectrum than a duality.* The pegs of our bodies come in many shapes but the sports world – and society at large – tries to squeeze these multiform and at times changing pegs into either square holes or round holes.
They lined us up outside a room where there were three doctors sitting in a row behind desks. You had to go in and pull up your shirt and push down your pants. Then they just looked while you waited for them to confer and decide if you were OK. While I was in line I remember one of the sprinters, a tiny, skinny girl, came out shaking her head back and forth saying. ‘Well, I failed, I didn’t have enough up top. They say I can’t run and I have to go home because I’m not ‘big’ enough.
Genetics entered the picture when the IOC Medical Committee introduced Barr body testing into the mix in the 1960s. In 1949, University of Western Ontario researcher Murray Barr and graduate student Ewart G. Bertram published a paper in Nature in which they demonstrated that, by using a simple staining technique, the chromatin of a cell’s inactive X chromosome in individuals with two X chromosomes could be identified with a microscope. In a methodology that might be ethically questioned by some today, Barr used feline neural cells obtained by brain biopsies of anesthetized cats. As every student of genetics knows, one X chromosome stays active and the remaining X(s) is inactivated in individuals born with more than one X chromosome. And, as every student of genetics knows, Barr body analysis is a less than perfect indicator of biological sex. Nonetheless, the IOC chose to use this analysis to determine who could or couldn’t compete in women’s competitions. It was a relatively easy test to perform at scale using buccal cells or (ouch!) hair bulbs.
Starting with the 1968 Winter Olympics in Grenoble, the IOC randomly tested some female athletes using Barr body analysis and sometimes Y chromosome fluorescence studies. In the 1968 Mexico City games, Mexican geneticists Alfonso León de Garay and Rodolfo Félix Estrada organized a large scale genetic testing program of 1,265 Olympic athletes and perform a wide array of genetic, cytogenetic, and familial studies in an effort to study the determinants of athletic ability. Their analysis included karyotyping but those specific results were not made available so it is unknown if any athletes were disqualified and how many actually underwent sex chromosome studies. By the 1972 Sapporo games, genetic testing of female athletes became mandatory (except for Princess Anne, sister of Queen Elizabeth, who, when she competed in equestrian events in the 1976 Montreal games, was given a pass on undergoing sex testing). Barr body analysis +/- Y chromosome staining continued until 1992, when they were replaced with SRY and/or DYZ1 PCR studies. As with Barr body and Y chromosome studies, SRY and DYZ1 status are also less than perfect predictors of biological sex. Some athletes “passed” Barr body testing in one Olympics only to “fail” the PCR test in a later Olympics. Sometimes you were female, and sometimes you weren’t, depending on the whim of the the rule makers and the available genetic technology.
Official reports of the Olympics used various names to refer to these genetic tests over the years: sex checks, sex control, femininity tests, femininity testing, femininity control, gender verification, gender testing, gender tests, and sex checks. Sometimes names fell into disuse only to resurface years later. This illustrates how changes in language norms often do not follow a straight-line trajectory, as well as confusion about distinctions between sex and gender, and just what it is the rules were trying to get at.
It’s unclear how many individuals were excluded from Olympic participation based on sex verification testing because the IOC didn’t always reveal that information and they wished to protect the confidentiality of the athletes, but apparently very few athletes were actually excluded, even if they “failed” the tests. Of course, some athletes may have been excluded by testing in their home countries before they were allowed to go to the Olympic Games and some Olympians may have quietly bowed out before the start of the Olympics if testing at the Olympics didn’t qualify them as women. By 1999, the IOC abandoned mandatory sex testing.
There are more instances of exclusion based on sex testing in non-Olympic competition, several of which received extensive and at times sensationalized media attention. In particular, some athletes were identified with differences in sexual development , and these athletes continue to pose the most controversial, challenging, and contentious situations for sports regulatory committees, athletes, the media, and the general public. Some intersex athletes were unaware of their conditions prior to testing. It’s tough enough explaining this information within the context of a genetics clinic to someone for whom there was at least a suspicion of an intersex condition. Imagine finding out for the first time just before a major athletic event and then sometimes having that information broadcast around the entire planet. Some athletes experienced serious psychological problems as a result.
Some in the genetics community expressed concerns about the use of these tests almost immediately. The objections raised by Albert de la Chapelle, Malcolm Ferguson-Smith, and the Singapore pediatrician/geneticist Wong Hock Boon, among others, were largely ignored. The Social Issues Committee of the American Society of Human Genetics also issued a report criticizing the use of genetic testing in sports. It’s unclear how much these objections influenced IOC policies. The IOC seemed to react more to social and media pressure than the opinions of physicians and scientists.
The IOC abandoned mandatory sex verification in 1999 and after two decades of changing rules recently produced a more fair-minded and inclusive policy following the Tokyo Olympics in 2021. However, the IOC leaves it up to the governing bodies of individual sports to determine who can compete as a woman. Many of these individual governing bodies use athletes’ testosterone levels to determine eligibility, as does the Women’s National Basketball Association and the National Women’s Soccer League in the US. Thus athletes such as Mokgadi Caster Semenya, Francine Niyonsaba, and Christine Mboma have been identified as intersex, and in some cases have been told they need to to undergo ethically questionable medical interventions such as gonadectomy or testosterone lowering drugs to compete in certain events. This can take deep physical and psychological tolls on interesex and transgender athletes, the ones who probably suffered the most from sex verification testing in athletic competition.
The general justification offered for sex verification testing is to level the competitive playing field. That is understandable and many athletes likely support that general concept. Fair compeition is, after all, why performance enhancing drugs are banned. However it is interesting that genetic testing was only offered for X or Y chromosomal material. There has never been routine testing for autosomal genes, such as some alleles of the EPOR gene, which can give an edge in marathon type sports by allowing the blood to carry more oxygen. The Finnish cross country skier Eero Antero Mäntyranta won 7 medals in 3 Olympics, possibly aided by his diagnosis of primary familial and congenital polycythemia (ironically he later tested positive for amphetamine, a performance enhancing drug). Although all of the genes linked to athletic ability have not been identified and is likely the result a complex interplay of many genetic and environmental factors, I am pretty sure the genomes of LeBron James, Katie Ledecky, Diana Taurasi (one of the most complete basketball players I have ever seen), and Lionel Messi look different than a lot of their competitors’ genomes, not to take anything away from these athletes intensive training regimens. But we don’t classify athletes by genotype – unless of course that genotype is related to biological sex.
The misuse of complex genetic information also occurs in non-athletic situations – MTHFR polymorphism testing, polygenic scores calculated for IVF embryos, ancestry testing to justify white supremacy, to name a few. No matter how hard geneticists try to shape the public conversation about genetics, once the CATG is out of the genetic bag, we have very little control over how it is reported, used, and misused. It plays out in social, political, legal, and ethical landscapes in unpredictable and at times harmful ways. It’s not merely a matter of better education of the public and various authorities. How genetics and other scientific information is used is shaped by prevailing ideologies, politics, and diverse cultural values. And sometimes by narrow-minded hate.
_______________________________________
– My favorite example of the non-duality of life is the green sea slug,Elysia chlorotica. In its juvenile stage it is brown with white spots and looks like, well, a slug. It seeks out specific algae –Vaucheria litorea – for food, and sucks out the algal cell’s contents, including the chloroplasts. The snail no longer needs food at this point, getting all of its energy from photosynthesis via the algal chloroplasts it ingested. Not only that, it transforms its morphology such that it eventually has a slug head but its body color changes to green and looks for all intents and purposes like a leaf, complete with veins. I first learned about E. chlorotica in The Light Eaters, Zoë Schlanger’s fascinating book that will challenge your ideas about plant life. Oh, and by the way, along the lines of trying to define biological sex, a green sea slug produces both sperm and eggs.
Medical geneticists and genetic counselors have an often complicated and at times tense relationship with people with disabilities, their families, advocates, and scholars. Geneticists are strong advocates and supporters for all of their patients, regardless of their abilities and disabilities. Although people with disabilities should not be viewed as a homogenous group with no variation in attitudes and beliefs, a visit to a genetics clinic can make patients feel very “other” when they are analyzed, catalogued, measured, and examined to determine just how different they are, to find out what’s “wrong” with them. Many patients and advocates – though by no means all – view prenatal testing as an existential threat. To better understand this situation, a look at the historical origins of medical genetics can shed some light on this dynamic.
The medical genetics specialty began to cohere and develop in the decades between the 1940s and 1970s. Its roots go back before 1940, mostly in the form of eugenics. The term “medical genetics” was introduced in the early 1930s*, likely independently, by the eugenics-minded Madge Macklin, then at the University of Western Ontario, at the 1932 Third International Congress of Eugenics and in 1931 in the UK by the vehement critic of eugenics Lancelot Hogben in his text Genetics Principles in Medicine and Social Science (although he proposed his own eugenic ideas in the text). But there was no clear cut profession of medical genetics or providers who called themselves genetic counselors in the early decades of the 20th century.
Lancelot Hogben’s text where he introduced the term “medical genetics.”
P. 214 from the Hogben text
Madge Macklin’s paper in which she introduced the term “medical genetics,” apparently independently from Hogben. Presented at the 3rd International Congress on Eugenics, New York City, 1932. Note the first sentence of the last paragraph, which states: “Until the medical practitioner is made aware of heredity as an etiological factor in the production of disease, he will not be apt to have a sympathetic attitude toward public education nor toward any scheme which may be devised to curtail the heavy economic waste of caring for the hereditary defective.”
The formative period for the medical genetics specialty began shortly after WWII ended. The first medical genetics clinics opened their doors in the 1940s and 1950s. The American Society of Human Genetics, the first professional organization for medical and other human geneticists, was established in 1948; its flagship journal, the American Journal of Human Genetics, first began publication in 1949. Accurate human karyotyping,** the primary genetic laboratory test for decades, became available during the 1950s, thanks to the work of Tjio and Levan. Several foundational texts were published, such as Victor McKusick’s Mendelian Inheritance in Man in 1966, Dave Smith’s Recognizable Patterns of Human Malformation in 1970, and Josef Warkany’s Congenital Malformations in 1971. The American Journal of Medical Genetics began publication in 1977. The American Board of Medical Genetics (now the American Board of Medical Genetics and Genomics), the original professional certifying organization for medical geneticists and genetic counselors, was incorporated in 1980. These achievements are hallmarks of a nascent profession working to establish its professional scope and legitimacy. They resulted in the creation of jobs, hospital departments, clinical laboratories, a research tradition, the profession of genetic counseling, and eventually contributed to the expansive growth of prenatal testing and commercial genetic testing laboratories.
Historians of science have offered several explanations for this post-WWII growth, such as increasing sophistication of genetic knowledge, an ethical reckoning with eugenics, advances in medical technology, and epidemics of teratogenically-induced fetal conditions such as fetal rubella syndrome and fetal thalidomide syndrome in the 1950s and 1960s. While these were contributing factors to the formation of the Medical Genetics specialty, I would argue that they were secondary rather than primary factors. Medical genetics was built primarily on the minds and bodies of people with genetic and congenital disabilities. Disability – and social attitudes toward it – was the initial raison d’être for medical genetics and the associated genetic counseling. Of course geneticists saw patients for indications other than disability. For example, a very common reason for referral to genetics clinics was to try to determine the ultimate racial appearance of an infant up for adoption so that it could be placed with a “racially appropriate” family. But the primary clinical focus of the early genetics clinics was the clinical evaluation of people with disabilities. No disability then no medical genetics (or at least a medical genetics that would have looked very different).
How can I make such a claim? Well, during this period there wasn’t much in the way of treatment for most genetic conditions. Instead, geneticists focused on describing the bodies of people with disabilities in painstaking clinical detail. Naming and identifying syndromes and their differences and sub-types. Determining the likelihood of a condition occurring or recurring. Describing anatomical structures that have gone embryologically awry. Measuring the distance between the eyes, the length of the philtrum, the distal phalanges, the head circumference. Noting the angle of the palpebral fissures, the insertion of the ear, the location of the anus relative to the genitalia. Commenting on the presence or absence of a single palmar crease, soft tissue webbing, fifth finger clinodactyly. How the bodies of people with disabilities were dysmorphic, malformed, deformed, and disrupted. In short, how their bodies differed from the “norm.” This gave medical geneticists a common vocabulary with which to communicate with one another, unique clinical skills, and it provided scientific legitimacy to their efforts. It also undoubtedly didn’t make people with disabilities feel good about their bodies. Nor would the stark clinical photographs published in genetics books and journals that sucked the dignity and humanity right out of the patients (often pictured naked and with their eyes blackened out).
This approach to patient care allowed the first waves of medical geneticists to establish their clinical expertise and carve out a professional niche that set them apart from pediatricians, neurologists, and other medical specialists. No other branch of medicine focused so heavily on parsing out human macro- and micro- phenotypic variation. A medical specialty was born.
Every medical specialty has its clinical focus, usually defined by specific diseases or organ systems. Oncologists treat cancer patients. Nephrologists care for patients with kidney disease. Cardiovascular specialists manage patients with heart disease. These patients were regarded as “normal” people with unfortunate diseases that needed to be treated and cured. People with disabilities were regarded as unfortunate people who needed to be prevented, reflecting prevailing social attitudes of this period. The genetic counseling provided during that time echoed these attitudes. Despite disavowals of eugenics, post WWII genetic counseling focused on avoiding the births of disabled bodies.
This is not to imply that medical geneticists during this period were bad people who intentionally and callously used the bodies of people with disabilities for personal and professional gain. These men (and they were almost exclusively males) were for the most part kind and compassionate physicians who cared deeply about their patients and usually treated them with respect and dignity, just like almost every medical geneticist I met throughout my career. Many patients were very grateful for the care they received in medical genetics clinics. It wasn’t a matter of bad physicians providing sub-standard medical care for devious purposes and personal gain. Rather, medical genetics was an outgrowth of the ableist and anti-disability structure of medicine and of society as a whole.
There was of course some level of reciprocity. People with disabilities and their families could benefit from the services provided by medical geneticists. A syndrome name to help end the Diagnostic Odyssey. Anticipatory medical and developmental guidance, referrals to neurologists, surgeons, educators, physical therapists, and other specialists who might treat and care for patients’ often complicated medical issues. A medical home where patients could make sure their often complex medical needs were being tended to and coordinated by a single care provider. An expert authority who could provide education and knowledge about often rare conditions that were beyond the clinical knowledge of pediatricians and other non-genetics providers. But the benefits were asymmetric. Patients and their families came away with perhaps recurrence risks, maybe a syndrome name, and some idea of what their medical and developmental futures might look like. But people with disabilities have managed to survive and live their lives since the dawn of humanity (though now always pleasantly) without the existence of medical geneticists. Medical geneticists, on the other hand, gained an entire profession. They needed the bodies of people with disabilities in order to create careers and a brand new medical specialty.
Medical geneticists today still care for patients with disabilities, though the situation is more nuanced and complex than in the past. Patients are generally treated with greater respect and have greater autonomy. Medical geneticists and genetic counselors have expanded their scope of practice to conditions beyond disability, such as cancer, neurological disorders, cardiovascular diseases, pharmacogenomics, and psychiatric conditions. Social attitudes toward disability are less negative than they once were and this is reflected in the way genetic counseling is provided. Genetic analysis has become more sophisticated. There are more treatment and management options for the health problems associated with genetic conditions, helping some people with disabilities and their families lead richer, healthier, and fuller lives.
Nonetheless, the historical tensions persist. Patients and providers often have different views of what constitutes a disability and what disorders need testing, treating, and curing. The list of conditions amenable to prenatal testing grows exponentially, usually with little or no input from the people and families affected by the conditions. The value of people with disabilities is often still measured in economic terms. Structural, conscious, and unconscious ableism is ubiquitous, even among the most sensitive and supportive providers and institutions. We’ve come a long way, but it’s still a long haul to go.
___________________________________________
* -The Macklin and Hogben references were the earliest I could find on the origin of the term “medical genetics.” If readers are aware of earlier references, please let me know.
** – Human, plant, and drosophila chromosomes had been analyzed since the early decades of the 20th century. However, the crude laboratory techniques did not always allow for accurate analysis or even correct chromosomes counts. The word karyotype was coined by the Soviet plant geneticist Grigory Livitsky around 1930. Like many Soviet geneticists of the Stalin era, Livitsky was arrested and eventually died in a Soviet prison in 1942 after ideological clashes with Stalin’s favored geneticist, the notorious Trofim Lysenko. Lysenko rejected Mendelian genetics and his scientifically misguided agricultural policies led to catastrophic crop failures, widespread famine, and millions of deaths in the Soviet Union and China, which also followed Lysenko’s lead. As with the Covid pandemic, millions of avoidable deaths resulted from a rejection of sound science and research.
In his poem American Sonnet Billy Collins compares a sonnet to “furrows in a small, carefully plowed field.” Classical sonnets are tidily structured works that more or less follow a format of 14 lines, often in rhyme, the last two of which offer a resolution to the problem or question set forth in the earlier lines.* The strictures and structure of a sonnet and the image of a plowed and furrowed field makes me think of how genetic counselors try to neatly organize genetic counseling sessions. The templated counseling notes we produce afterwards – some version of Patient Identification, Medical History, Family History, Counseling Provided, Summary and Recommendations – reinforce the idea of a structured session as well as the sonnet metaphor.
We try to impose structure, for reasons both good and not so good. In many clinical positions, most patients are coming to us with a handful of similar indications such that we wind up saying more or less the same things over and over, especially when we carry large patient loads. My roteness would become clear to me when a patient “interrupted” me with a question about something else altogether and I would forget where I was in my game plan. I was not listening to the message the patient was sending – they were not much interested in what I was talking about and they wanted to discuss something more important to them. Genetic counselors, with our professional insecurities, also subconsciously want to impress others with our arcane knowledge and prove that we can make an important contribution to the health and medical care of patients and their families. This manifests itself most acutely during the early stages of a career, when we are still slightly unsure of ourselves and are trying to establish a firm professional footing and reputation. But even wise veterans can get caught up in this style, including and particularly me (well, not anymore, now that I’ve converted to my favorite religion – Reitrementism).
While acknowledging the important role that numbers and information play in genetic counseling and patient care, a counseling session is at its core a psychological interaction between human beings. It took me – no kidding – a couple thousand counseling sessions before I even started to become a good genetic counselor and adapted my counseling to the basic psychological truth that the human mind usually expresses its emotional self in a non-linear manner. I knew this on a cognitive level but it took me years to actually incorporate this insight into my practice. To paraphrase Maya Angelou, people won’t remember what you said but they will never forget how you made them feel.
What does this mean in actual genetic counseling practice? I’m not advocating for omitting facts and figures or abandoning an over-arching loose structure. A counseling session should have a beginning and ending, and complex biomedical information often needs to be imparted. You can start out with a highly flexible plan of issues and information you think should be covered while at the same time be very willing to modify the plan or abandon it altogether to meet the unique needs of each patient. It might begin with a query as to what the patient wants to get out of the session, though some patients are better at articulating that than others and some just aren’t sure of what they want. But however you start, you need to be prepared for traveling with the patient as they veer off in often unclear directions that are sometimes different than what the patient originally articulated. Structure, numbers, information – they are so comforting and comfortable to us, like Collins’ neatly furrowed fields. But the safe zone of an organized educational format can make us hesitant to explore the unplowed fields of the patient’s psyche.
What we can discover in those unfurrowed fields is what is important to patients, why it is important, and how it influences the way patients makes sense of complex biomedical information and what they should do with it. Fear of going through treatment for cancer after having watched their parent’s body ravaged by chemotherapy. Anger at an employer for creating an emotionally or physically toxic workspace and attributing their cardiomyopathy to this environment. A deep belief in “natural cures” that is being challenged by their lack of efficacy in treating their child’s illness. Feelings of abandonment and resentment toward a parent who died when the patient was an adolescent and who is now a parent of an adolescent themselves. Fear of having a child with a disability. A marriage adrift on two different seas. Distrust of medical practitioners stemming from having been treated disrespectfully in past encounters. All of the technical information can be so damn scary they don’t want to talk about recurrence risks or the chances of getting cancer or variants of uncertain significance, at least not right away and not by listening to what sound like a verbal spreadsheet. Genetic counseling is supposed to make the patient feel emotionally safe, not the counselor.
What this requires is actually attending to what the patient is saying or asking, especially if it has little to do with what you are discussing. You don’t want to briefly comment on what sounds like a non-sequitur from the patient and then return to the safety of your comfortable structure. Following the patient’s lead can result in a session which travels in several different seemingly unconnected directions (Why is the patient going off at this angle?), loops back on itself several times (Hmm, why does the patient keep coming back to that?), or has you probing the patient with questions neither of you had anticipated (“And so you’re saying MRIs are scary to you because you have claustrophobia and you’ve also read that the MRI’s magnetic field is thousands of times stronger than the earth’s magnetic field at its surface, and that’s why you are reluctant to undergo hereditary cancer testing?”). It can become a near stream of consciousness session that resembles James Joyce’s Ulysses more than Elizabeth Barrett Browning’s tenderly romantic How Do I Love Thee?. Joyce’s novel begins with the famous opening line that seems to presage a typical narrative – “Stately, plump Buck Mulligan came from the stairhead, bearing a bowl of lather on which a mirror and a razor lay crossed.” – then quickly changes tone and explores the depths of the minds of the novel’s characters and ends with Molly Bloom pouring out her innermost thoughts in an unpunctuated iambic-pentameter-be-damned eight sentence ~22,000 word uninhibited and unfiltered soliloquy. Kinda’ like a counseling session can go (Nothing against Barrett Browning. She is a marvelous poet; just a different style than Joyce’s).
I don’t know how AI chatbots will play out in the genetic counseling arena and how they might influence the structure of genetic counseling sessions. It seems possible that they might one day be capable of carrying out a psychologically sophisticated interaction with a patient that matches a counselor’s skill set as well as taking into account the patient’s socioeconomic situation, though I suspect not in the immediate future and hopefully not until the ethical issues have been addressed (for an amusing take on chatbots and genetic counselors, check out my post Genetic Counselor Reinvented). My bigger immediate concern is that administrators will simply see chatbots as a replacement for genetic counselors rather than as an ancillary tool for genetic counseling. Or that administrators will employ a strategy that employs both genetic counselors and chatbots but increases counselors’ patient loads on the premises that chatbots are doing a lot of the work and so you can fit more sessions into a counselor’s schedule. This ignores the emotional toll on genetic counselors who work with patients in stressful situations and will likely lead to counselor burnout and poorer quality patient care.
The potential and concerns about AI aside for now, the semi-chaotic session is often more valuable to patients than the biomedical lecture. Yeah, it can look and sound like a mess and be just as dense and difficult to understand as Ulysses. But that mess is where the beauty of the patient’s mind lies. Which is why we need to use our counseling skills to sort through the mess and understand the psychological meaning of the patient’s words, beliefs, actions, and choices. Hence the wonderful messiness of genetic counseling.
The Brain — is wider than the Sky — For — put them side by side — The one the other will contain With ease — and You — beside — by Emily Dickinson
Over the centuries, poets have played with the format of the sonnet to breathe new life into it, such as Wanda Coleman’s American Sonnet 91 and other of her decidedly non-linear poems that explore race and racism in America.
Polygenic risk scores* are all the rage these days. Thousands of articles and research studies have attempted to link polygenic scores to just about every medical condition, behavior, and trait you can think of, and a few I had not thought of such as reproductive behavior. They have contributed to improving our understanding of human genetic architecture, hold potential for guiding treatment decisions, and have started to open the black box of gene-environment interplay, to name a few applications. Polygenic scores have laid bare the racial/ethnic bias in genetic data bases that have proven to be overwhelmingly comprised of people of Northern and Western European ancestry and shamed the genetics community into striving to better serve all communities. They have also been used inappropriately in clinical practice, such as with preimplantation genetic testing to predict potential height and intelligence of an embryo (quite poorly as it turns out) to determine its “implant-worthiness.”
The value of polygenic scores in clinical settings, despite the optimism expressed in many of the publications, remains unproven for the most part. Time and more research will presumably filter out the clinical winners from the losers. But we also need to sort through the thorny ethical, economic, and social justice issues with equal intensity and resources.
One particular application of polygenic screening is undermined by a naïve understanding of human psychology and a failure to learn from past experience in genetics – population polygenic screening for common conditions such as cardiovascular disease, diabetes, hypertension, and cancer. I don’t believe that polygenic scores will have a particularly strong impact on reducing the impact on morbidity and mortality from these common conditions. There is ample evidence that genetic testing has little or no effect on risk-reducing behaviors. In fact, I’d go as far to say that the research investment into population polygenic screening for these conditions is disproportional to their likely medical benefit.
The aim of polygenic screening for health conditions is to produce a number, some likelihood that a healthy person will eventually develop condition X, and that risk estimate would be the basis of medical recommendations to reduce or manage the risk. As with all likelihood estimates in clinical care, polygenic screens, with or without inclusion of demographic and clinical variables, will be imperfect, maybe slightly more or less imperfect than estimates derived by other means. Genetic counselors have been dealing with such numbers since we first entered clinics half a century ago and began providing patients with empirical recurrence risks for genetic conditions or the probability of having a baby with an aneuploidy based on parental age or screening results. Some think that providing numbers is the purpose of genetic counseling but it turns out to be only the beginning of the counseling session (emphasis on counseling).
The naïve assumption underlying polygenic screening for common conditions is that the risk number will magically motivate people to undergo more frequent colonoscopies, breast MRI, change their diet, stop smoking, exercise more, and reduce the stress in their lives. Yeah, well, good luck with that, at least on any large scale, on a sustained basis, and outside the context of a research study of self-selected participants conducted over a short time span. Sure, some people will be nudged into screening uptake or lifestyle changes, and a smaller percentage may even keep it up. But decades of experience have shown that most people are going to continue doing what they are doing with their lives – healthy behaviors or not – thank you very much.
There is a persistent but mistaken view in genetics, and medicine in general, that the human psyche is an objective statistical risk calculator and the “right” number will motivate people to do the “right” thing. This is a zombie concept that, like nondirectiveness, refuses to die. But the human mind is a complex and not entirely rational system, at least not like a Sherlock Holmes ratiocinative detective type of rationality. Numbers are embedded in a patient’s psychological, emotional, life-history, social, economic and political matrix that can vary over the short and long term. Numbers are interpreted or misinterpreted or denied or ignored such that it fits into the patient’s elastic view of the world. The results are often decisions that seem to make no sense or appear ludicrous to medical professionals but makes perfect sense to patients at this point in their lives. That decision could change over time, sometimes for apparent reasons such as the death of a family member, and sometimes for no obvious reason. They can even change from a “good” decision to a “bad” decision.
Of course, some people seem to be nominally objective decision-makers, the so-called engineer or statistician types. The patients who suddenly become actively engaged in the genetic counseling session once numbers are tossed out for discussion, dissecting and closely questioning their accuracy, how they were derived, and what the confidence intervals are. If you bring up statistical measures such as area under the curve or Cox proportional hazards, they even seem mildly sexually aroused. But the engineers and statisticians ultimately interpret numbers psychologically, just like the rest of us.
I don’t mean to imply that polygenic scores are totally useless. One of our jobs in medicine is to find ways to reduce the impact of disease on patients’ lives and polygenic scores might provide some help to that end. Research into polygenic traits can contribute to the scientific understanding of human and medical genetics. And polygenic scores will likely have some clinical utility. I can see some settings where a health risk has already been identified and a polygenic score can help further refine that risk. For example, polygenic scores might modify the ovarian or breast cancer risk or the age of onset in a patient who carries a pathogenic BRCA1 variant. It could then influence timing of risk-reducing surgeries or help determine if such surgeries are even necessary. Readers can undoubtedly think of other scenarios where polygenic screens might help influence decision making by high risk or affected patients.
We need to scale back expectations that population polygenic screening will significantly reduce the morbidity and mortality stemming from common conditions. I suspect that its impact on disease and death will be modest and at times unclear, perhaps with an occasional success story. The minimal research that has been done to date on the uptake of screening or other medical recommendations after a polygenic screen have produced mixed results and are not overwhelmingly convincing, though of course further research may prove otherwise.
There are also technical reasons to suspect that polygenic screens may not work well on a population level as measured by detection rates, false positive rates, and positive predictive values. In addition, existing inequities in access to and utilization of health care will further reduce the utilization of polygenic scores and subsequent follow-up of medical management recommendations by patients. If you don’t have access to good medical care and the appropriate interventions, or you can’t pay for it, or you have a lack of trust in the system, what good is screening?
Figure 2 from Hingorani AD, et al, BMJ Medicine 2023;2:e000554. doi: 10.1136/bmjmed-2023-000554Performance in screening estimated for polygenic risk scores included in the Polygenic Score Catalog from April 2022. Limits of each box represent interquartile range and horizontal line within each box is estimated detection rate for a 5% false positive rate (DR5) based on performance metrics reported for corresponding polygenic risk scores. Selected diseases are colour coded into categories cancers, cardiometabolic conditions, ocular diseases, allergic or autoimmune diseases, bone disease, and neuropsychiatric diseases. Horizontal line is estimated median DR5 value based on performance metrics for all 926 polygenic risk scores and all diseases studied in the Polygenic Score Catalog.
We need to take a hard look at just what we expect to achieve with polygenic scores. A lot of energy, resources, and finances go into research and publications about polygenic screens. Perhaps that time and money could better be directed to research where benefits of polygenic testing are more likely to be realized or to other areas of genetic research altogether, like how and why people make decisions about healthcare and how it is affected by personal, economic, social, historical, and political factors (think Covid vaccination uptake).
The medical genetics community may be resistant to my recommendations. Some of that resistance will be based on thoughtful and understandable disagreement with my opinions and their own assessment of the potential of polygenic scores in a population setting. But underlying some of that disagreement, and some of the enthusiasm for polygenic scores, is that all the players in the genetic testing game have blind spots and conflicts of interest. Researchers in the academic/clinical research industrial complex need grants and publications to further their careers. This includes not only Principal Investigators, but also the many other people necessary to conduct research – ethicists, research assistants, junior investigators, etc. The genetic counseling profession has for better and worse taken up genetic testing as its defining role in the medical system, and genetic counselors working in direct patient care demonstrate their economic worth to their employers by increasing the downstream revenue that results from genetic testing (revenue raised directly by genetic counseling alone is rarely enough to cover salaries and benefits). Commercial laboratories make their money by selling genetic tests; not a bad thing in and of itself but it can cloud one’s views. With all these players all talking the same game, they can lose sight of what’s good for the fans and unintentionally prioritize what’s good for the teams, such as citing improving institutional revenue from increased imaging as one of the benefits of polygenic scores or direct-to-consumer commercial labs offering polygenic scores when the health benefits remain at best unclear. I am not suggesting that researchers, genetic counselors, and labs are unethical and I am not questioning their dedication to quality medical care for patients. They are just being human and the human mind has a way of persuading itself that it’s doing the noble thing when in fact it may be putting its own interests first.
People interpret numbers how they want to interpret them. We see evidence of this on a large scale every day. Climate change is ignored in the face of rising temperatures and melting ice packs. Election results are denied because they don’t conform to the desired outcome. Millions of pandemic deaths are explained away as falsified or manipulated numbers to justify disregarding public health measures. This holds equally true for the results of genetic testing in populations. If we want genetic testing to be useful to our very human patients, we must develop a more sophisticated and less naïve understanding of the human psyche.
* – There is some controversy about the name “polygenic risk score.” “Risk” tends to evoke anxiety in our minds; typically, one is not at risk for good outcomes, like winning a large lottery prize. It also implies a value judgment on the condition being screened for. Many people would argue that deafness or autism are desirable or normal outcomes, not something that one is at risk for. Alternatives include “polygenic score” or “polygenic index.” I like my own coinage – “polygenic screen” – when referring specifically to polygenic risk scores for medical conditions in healthy people since it implies the test is not diagnostic (yes, I know, people tend to confuse diagnostic tests with screening tests à la NIPT). In this posting, I use all these terms more or less interchangeably because, well, I can’t make up my mind which I prefer.
In order to distinguish between the various applications of polygenic scores, consider these suggestions for a possible terminology:
Polygenic Index – when used to predict a non-medical trait, such as height or intelligence.
Polygenic Screen – when applied to population screening for common medical conditions.
Polygenic Risk Score – when applied to a population previously identified as being at high risk for, or affected by, a medical condition, such as breast cancer, to potentially guide treatment, risk reduction, and surveillance recommendations.
To distinguish between a polygenic only model and a model that combines SNP analysis with clinical and demographic factors, a “+” could be added, e.g., Polygenic Screen+– Breast Cancer to denote a breast cancer risk prediction model that incorporates SNP analysis with the Tyrer-Cuzick or other breast cancer risk prediction model.
The collective memory of eugenics is that it was an ideology of archconservatives that thrived during the first half of the 20th century and whose demise was hastened by the horrors of Nazi Germany. We like to think that we now know better. Better science, better morals, better guiding ethical principles. Heck, we must even be better people. It may be a comforting story, but historians of science have been pointing out for decades that this collective memory is flawed. Eugenic ideologies and policies, usually under different labels and in various forms, can be found today in science, medicine, and social policies.
Strands of eugenic beliefs also became embedded into popular culture. For example, as historian of science Paul Lombardo has demonstrated, references to eugenics could be found in the advertisements of popular magazines and newspapers in the first half of the 20th century, suggesting that the average American was familiar enough with eugenics that the term needed no explanation. For marketing purposes, eugenics implied excellent consumer products such as diamonds, hair styles, and hair shoes, in much the same way that many companies today will state that the quality of its products or the company’s dedication to customer service is part of the company’s DNA. There are many other examples of eugenic themes in 20th and 21st century novels, films, comics, and video games.
Along these lines, I recently came across two Walt Disney cartoons that echo eugenic themes. I couldn’t believe it at first. I thought maybe it was just my hyperactive eugenics paranoia kicking in and deluding me. After all, I tend to see eugenic monsters lurking under my bed at night. But the more I studied the cartoons, the more convinced I became.
Disclaimer: I have no reason to believe that Walt Disney himself was a dyed-in-the-wool eugenicist or that the Walt Disney Company is a front for a nefarious eugenics media empire. Rather, these cartoons illustrate how eugenic ideology was so pervasive that it subtly and not so subtly became woven into the fabric of American popular culture. It could appear in a cartoon without the creators having a single eugenic bone in their body. Or it could manifest under a different name, so disguised that a cartoonist might not recognize it for what it was.
The first cartoon, Goofy’s Adventure Story from 1954, tells the story of the family history of the Disney character Goofy. Goofy is an anthropomorphized dog who first appeared in 1932 – the heyday of classic eugenics – as the character Dippy Dawg. The cartoon includes a family tree in reverse order of tree growth, i.e., with the ancestral Caveman Goofy at its apex and 1950s Goofy at its base (which, curiously, is how family trees were typically drawn until about the 15th century). Descending between the two is a lineage of historical Goofy characters. Each ancestor is basically a stereotypical White European (for the moment, ignoring Goofy’s canine heritage*). In the cartoon, each character does something, well, goofy, in keeping with the character’s namesake trait. Goofy appears to be part of a patrilineal society since there are no female ancestors on the tree.
The family tree was a powerful symbol for eugenicists, who recognized the value of graphics in getting their point across. The many pedigrees of “feeble-minded” families produced by eugenicists were used to “prove” that intelligence was inherited in Mendelian fashion and that the people at the lower end of the intelligence spectrum were breeding at such incredible rates that the very existence of society was threatened by their reproductive drive, low intelligence, and propensity to crime and poverty. The pedigrees of “feeble-minded” families – typically poor and from “degenerate races” – reflected the race and class biases of eugenicists, who were primarily economically well-off Northern and Western White men.
Goofy’s family tree is a variation on these eugenic pedigrees. Goofy’s tree is peopled with Noble White Man tropes so beloved by eugenicists, such as Roman emperors, Greek warriors, knights in armor, and Pilgrims. In keeping with Goofy’s nature, these figures are presented in comic form. But the comic form gets at the essence of the connection to eugenics. Think about it for a moment – the name Goofy is synonymous with “feeble-minded,” a connection reinforced by his signature “Hyuk, Hyuk” laugh and two widely-separated upper teeth (which don’t look like canines to see). Disney, of course, wasn’t trying to revive classic eugenics. Rather, Goofy’s pedigree illustrates how the eugenic notion that intelligence was inherited and ran for generations within families was so engrained into the public consciousness that, even without thinking about eugenics. it was natural to create a “feeble-minded” cartoon character who has a family tree full of “feeble-mindedness.” Goofy’s family history is a modified and cartoonized version of the pedigrees of the Jukes, the Kallikaks, the Hill Folk, the Mongrel Virginians, the Pineys, the Nam Family, and the many other “degenerate” families described by eugenicists.
A rendering of the Kallikak Family tree from a 1950s psychology text (contemporaneous with Goofy’s family tree), based on the 1912 book “The Kallikak Family: A Study in the Heredity of Feeblemindedness” by Henry Goddard.https://en.wikipedia.org/wiki/The_Kallikak_Family
The Goofy family tree also includes an odd appendage, one that I have decided to believe is unintentionally inappropriate and reflective of what was considered acceptable at the time rather than a, uh, racist dog whistle. Dangling from the lowest branch on the left is a noose. I am not exactly sure what a noose is doing here although I guess it’s somehow connected to Wyatt Earp Goofy, who appears to be nailing a Wanted poster to a tree. Not that I expect a cartoon to be historically accurate, but Earp is not particularly associated with hangings, and in fact helped disperse a mob that was intent on hanging a man accused of murder. The noose, of course, is an image used by White supremacist racists to try to strike fear in the hearts of Black people in America. Along these lines, in the cartoon Wild Bill Goofy shoots a Native American in a manner that’s somehow supposed to be humorous, and the appearances of Native Americans and South Seas “cannibals” are depicted stereotypically.
In another weird twist, the country the Goofy Family Tree appeared on a postal stamp issued by Uganda in 1992, celebrating the 60th anniversary of the creation of the Goofy character (Disney characters were licensed for use on postage stamps in many countries).
In the other eugenic-themed Disney cartoon, titled Family Planning, Donald Duck helps a disembodied narrator explain family planning. The cartoon does not detail the specific methods of family planning other than “taking pills” and “using simple devices.” Just as well, I guess. I for one was not interested in Donald Duck demonstrating how to use a condom or Donald and Daisy practicing the rhythm method.
Some of the Population Council’s early presidents had strong ties to pre-World War II eugenics, most notably Frederick Osborn. Osborn helped create the journal Eugenics Quarterly, was a founding member of the American Eugenics Society and a member of Britain’s Eugenics Society, and once characterized Nazi eugenics as “an important experiment.” After WWII, he apparently had a fall-off-his-ass experience and began portraying himself as a severe critic of classic eugenicists such as his uncle Henry Fairfield Osborn. He shifted his focus to positive eugenics (i.e., encouraging the “right” people to breed and encouraging the “wrong” people to voluntarily curb reproduction) and acknowledged the role that environment played in an individual’s development and lot in life, what might euphemistically be called a kindler, gentler eugenics.
Despite Osborn’s claim to the contrary, these two quotes from 1965 and 1963, respectively, demonstrate that he had not fully shed some of his hard core eugenic beliefs:
…the average genetic character of parents of unwanted children is likely in the long run to be below average. An unusual proportion of these unwanted children grow up to be juvenile delinquents, unemployed, or social charges.
Every racial group has a certain proportion of genes for high ability…. It appears that ever since World War II, Negroes as a group have been increasing in numbers more rapidly than the Whites, with a probable trend during this period towards producing relatively fewer able individuals. This is the kind of dysgenic situation which eugenics aims to ready.
Osborn was no longer president when the cartoon was produced and as far as I know did not play a role in developing it. But his eugenic philosophy strongly influenced the organization’s policies during the 1960s. It’s this Osbornian view of humanity that guides the message of the Disney cartoon.
The cartoon’s central character is a peasant farmer with a skin tone a shade or two darker than white and who speaks English with what sounds to me like a Central American accent. When the family has only 3 children, the farmer is able to provide for his family – enough food, schooling, and a few simple possessions such as a radio. But, according to the cartoon, if the family goes on to have 4 more children, the farmer will no longer be able to provide enough food or otherwise meet the basic needs of his family. The parents become so tired they can barely care for their children, who grow weak and sickly. When the sons grow up, the small family plot will have to be divided among them, restricting their ability to care for their families. Heaven forbid, should the family move to the city they will be even worse off because they can’t afford to live there. The narrator’s solution is for the peasant to practice family planning so that reproduction is not “left to chance” and “you can only have the children you want.”
Eugenic themes were not confined to cartoons. They can be found in other areas of popular culture from that era and even up to today. The Beverly Hillbillies (“a poor mountaineer who barely kept his family fed”) are the cultural descendants of Charles Davenport’s Hill Folk. As are the inhabitants of the hills of northern Georgia in James Dickey’s novel Deliverance (“Nobody worth a damn could ever came from this place.”) who terrorized the rich urban men seeking to display their manhood by spending a weekend rafting a wild river. Or, from a previous generation, the immigrant-hating horror novelist H.P. Lovecraft who wrote of unimaginable alien horrors lurking in the hills of New England (“West of Arkham the hills rise wild… When I went into the hills they told me the place was evil.”). In a clever thematic manipulation, the current TV series Lovecraft Country features Black characters facing the monsters of White racism across America’s 1950s South.
The current spate of zombie movies, novels, and television shows can be read as eugenic, with their mutated throngs of human monsters threatening the existence of Western civilization. Perhaps it’s no coincidence that the popularity of the zombie genre is blossoming during a time of anti-immigrant sentiment in Europe, America, and other places. Eugenics has an uncanny ability to morph and adapt to different times and different cultural milieus. And, like zombies, it refuses to die.
– Someone really should perform whole genome sequencing on Goofy and Pluto to finally resolve the long-standing debate about the differences between the two, Goofy being a canine who is bipedal, language fluent, and a friend of Mickey Mouse whereas Pluto is a quadrupedal canine, incapable of speaking, and is Mickey’s pet. Surely the difference lies in their genomes.
At the recent NSGC Annual Conference, Carla McGruder chaired a sparkling plenary session titled “Say My Name, Say My Name”during which panelists debated the pros and cons of the professional title Genetic Counselor (there was widespread disappointment that Beyoncé did not make a guest appearance). The general sense I got from the debate was that there was enthusiasm for a name change and that a new professional title may ultimately prove to be destiny’s child, but for now no one offered a particularly winning alternative (see below word cloud from the session). Perhaps unsurprisingly, nobody brought up my two biggest long-standing concerns about the genetic counselor title. One is that the oft-used abbreviation of GC for genetic counselor is also the abbreviation used for gonococcus bacteria (though then again it could also more appropriately suggest guanine and cytosine). My other concern is that we should more properly be called genetics counselors; genetic counselor without the “s” at the end of genetic makes it sound like being a counselor is a hereditary condition, the result of some likely pathologic variant. I am pretty sure, too, that lots of genetic counselors in Canada, the UK, Australia, and some other countries would prefer everyone spell it “genetic counsellor.”
Word Cloud for suggested alternative professional titles for genetic counselors, from “Say My Name, Say My Name” panel discussion at the NSGC’s 42nd Annual Conference in Chicago, October 20, 2023. Reproduced with kind permission of session chair Carla McGruder, MS, CGC.
Debate about what to call ourselves has surfaced with some regularity since the profession was birthed a half-century ago at Sarah Lawrence College, and in a journal article by Jehannine Austin and their group at the University of British Columbia, as well as being the subject of two prior DNA Exchange postings, one by my DNA Exchange colleague Allie Janson Hazell and one by me. I suspect that currently the name debate is driven by the profession’s expansion into so many new employment niches, many of which do not involve direct patient care. It may also be influenced by the increasing trend of the profession defining itself – and being defined by other health professionals – in relation to genetic testing.
Let me state my biases up front. I am opposed to a name change, at least until you can show me something better that will justify the very extensive, expensive, and intensive efforts of introducing a new name and eliminating an old one. Of course, my biases are partially driven by being an Old School GC, having graduated in the Late Neolithic Period of genetic counseling, back in 1983. There’s always the attitude of “Damn it, the way I was taught is the right way.” And even if someone comes up with a better job title, I will still likely go to my grave calling myself a genetic counselor. But my personal hang-ups and emotional reactions aside, let’s take a look at some of the pro arguments and why I think they fall short.
One of the pro arguments for a name change centers on lack of public awareness of just what a genetic counselor is or does. Yeah don’t we all know that one! I can’t disagree with this point. But changing our name will not in and of itself improve public awareness or visibility. The alternative names are equally or more ambiguous. Patients will probably react with uncertainty to titles that include the likes of analyst or consultant or specialist (to name just three) and it will do nothing to clarify how we might help and serve them.
While acknowledging the general lack of public knowledge about genetic counselors, we have nonetheless made remarkable progress in increasing awareness of the job title, both with patients and healthcare providers. The below Google Ngram, with all of its limitations, gives a rough idea of how much awareness of genetic counselors has increased since Sheldon Reed christened us in the 1940s, with the ambiguous but reasonably accurate definition of “a kind of genetic social work.” A lot of that progress can get lost if you eliminate the genetic counselor title.
If you really want to improve public awareness, you have to think beyond name changes and PR campaigns. Look at what the Dr. Jennifer Melfi character in The Sopranos did for publicity for therapists. What we need is a successful streaming series about genetic counselors, complete with gratuitous sex and nudity (we can hold off on the violence; there’s more than enough of that to go around in the world these days). I can picture the genetic counseling show’s log line: “Family Lines” – Follow the professional challenges, joys, tragedies, and dilemmas as well as the complicated personal lives of young, attractive, ethnically and gender-diverse genetic counselors as they graduate from their training programs and experience the impact of genetic conditions on their patient’s lives and families as well as on the counselors’ own psyches. Starring George Clooney as the dashing veteran Robert “Bob” Resta whose efforts to guide this gaggle of counselors throughout their careers are undermined by his own very human failings.Consider running the credits over a background of a pedigree being drawn to highlight the commonly used genetic counseling tool and to evoke the name of the show.
Proponents of a name change quite rightly claim that the term “counselor” doesn’t reflect what many genetic counselors actually do in their day-to-day work. Genetic Counselor does not capture the essence of a Variant Analyst, Professional Support Specialist, Product Development Manager, Program Administrator, Researcher, or Medical Science Liaison. But, according to the 2023 NSGC Professional Status Survey, 71% of genetic counselors are involved with full or part-time direct patient care. This suggests that a significant majority of us are actively engaged in genetic counseling on a regular basis, so it makes sense to call us genetic counselors.
Besides, the proposed alternatives capture an even smaller range of what genetic counselors do for a living or otherwise sell our skill set short. For example, one of the suggested alternatives is something along the lines of Genetic or Genomic Information Specialist. It strikes me that the word “Information” misses a critical insight into the human psyche. It isn’t so much the information that’s communicated that is key as it is the way that each person’s mind uniquely interprets that information and integrates it into their lives. this is where counseling skills come in, which, for my money, is what sets the profession apart and makes it uniquely valuable. It gives us a professional identity unlike any other genetics profession or specialty. The value of counseling and communication skills is acknowledged by many genetic counselors employed in non-direct patient care positions, who often claim that their counseling and communication skills have been key in enabling them to expand into their new roles. They are still using basic genetic counseling skills, just in a different context.
Furthermore, I would argue that the very ambiguity inherent in the genetic counseling title is what has allowed us to grow our professional roles. Other professional titles might not provide the flexibility to expand into new and exciting roles. If employers are not exactly sure of what we do, it allows us create new roles that other providers don’t have the knowledge base or skill set to match. As Ed Kloza – who has pretty much witnessed the entire history of the profession first hand – sagely pointed out at the microphone at the “Say My Name, Say My Name” session, the title genetic counselor has gotten us pretty far professionally since the 1970s. Just how has it limited us?
A decidedly practical drawback to changing our professional title lies in the bureaucratic underpinnings necessary to maintain the life of a profession. It’s not just a name that can simply be eliminated by a search-and-replace function. The title Genetic Counselor is written into state licensure laws, pending federal legislation to make genetic counselors recognized Medicare providers in the US, and other countries’ equivalents of licensure. To say nothing of changing job titles by every employer of genetic counselors, the names of a half dozen or so professional organizations, a journal title, and a PubMed search term, to name a few. This could potentially be achieved but you need a very, very compelling reason to expend all that energy, time, and money doing so.
It will be interesting to see what what happens with the job title in countries where the genetic counseling profession is just establishing itself – such as India, the Philippines, and the Middle East. Local circumstances, medical practice, and cultural preferences may wind up generating some very different names and professional practices. But I suspect that they may also want to stick with the genetic counselor title to capitalize on the remarkable progress the profession has made in the US, the UK, Canada, Australia, and elsewhere. The practice and profession may look a bit different around the globe, but they will still be recognizable as genetic counselors and not as something else.
Perhaps too, it is time to reconsider the 2006 standard definition of genetic counseling. While I happen to be a champion of that definition, my professional conflict of interest is that I helped craft it. The current generation of genetic counselors should not necessarily have to rely on a definition created by a previous generation if it no longer captures the essence of genetic counseling. This could have bearing on whether we should choose a new professional title.
For now, though, Genetic Counselor may be a less than perfect name but it is closer to perfect than the proposed alternatives. Give me powerful reasons to think otherwise, and I will change my mind. Until then – Change my name? Nah.
What is the economic worth of one person’s life? That question was raised yet again in a recent paper on expanded carrier screening (ECS) that justified an expanded carrier panel based on the cost-savings garnered by avoiding the birth of people with any of 300 mendelian disorders. A quick and likely incomplete literature search revealed other similar publications from around the globe (Azimi et al., 2016; Beauchamp et al., 2018; Busnelli et al. 2022; Clarke, 2021; Wang et al., 2022). NSGC’s Expanded Carrier Screening Guidelines also point to economic gains as one of the benefits of carrier screening. Other professional guidelines and research papers do not discuss the economic benefits of expanded carrier screening, though read carefully, the disability avoidance/cost savings theme is often an undercurrent. To me, economic justifications for ECS raise serious concerns.
The quantification of saved costs over time will help to critically examine the medical necessity of ECS as a proactive health screening strategy. – NSGC Expanded Carrier Screening Guidelines,2023
To be clear, I don’t object to carrier screening per se and a “pan-ethnic” panel can make more sense than an ethnic-focused panel. All patients deserve the right to make complicated and highly situated reproductive decisions and access to genetic testing should be fair and equitable, points which most professional guidelines agree on. My concerns arise from the purported economic benefits of ECS through disability avoidance (I, along with Katie Stoll, have some other concerns about ECS besides economic cost benefit analysis).
But first some historical context.
During medical genetics formative decades in the mid-20th century, the concept of cost-savings by preventing the birth of people with genetic conditions was baked into the field, using ingredients leftover from eugenics. Many leading geneticists at the time preached about the economic and other costs to society of genetic mutations (and by extension, the worth of people who carry such pathologic gene variants), and how it was important to eliminate these pathologic variants to save society money and to preserve the future of humanity itself. While post-World War II geneticists typically disavowed old school eugenics, many of their concerns continued to echo the field’s eugenic origins.
Let me illustrate this history with a notable example. In 1954, the National Academy of Sciences formed a group called The Committees on The Biological Effects of Atomic Radiation (often called The BEAR Committee), six separate committees that were charged with reviewing the available data on the range of biological effects of atomic radiation. A 1960 report from this group detailed the findings from the Committee on Genetic Effects of Atomic Radiation. The genetics committee was comprised of some of the leading brilliant geneticists of the day – George Beadle, Bentley Glass, James Crow, Theodosius Dobzhansky, Herman Muller, James Neel, and Sewall Wright, to name a few. Sewall Wright, in his chapter in the report “On the Appraisal of Genetic Effects of Radiation in Man,” divides humanity into 13 groups, based on intellectual, behavioral, and physical traits. Wright then decides the degree to which each category’s contribution to society is greater or lesser than its cost (as far as I can tell, based on Wright’s opinion and zero data). Some examples of these categories give an idea of their flavor:
1. In the first category, which includes the buIk of the population, there is an approximate balance between contribution and cost, but both at relatively modestlevels.
4. In this category are those who cost society much in term of education and standard of living but who contribute much more than the average at their level of cost.
6. We may put here individuals of normal physical and mental capacity whose cost to society outweighs their contribution because of the antisocial character of their efforts: charlatans, political demagogs, criminals, etc.
8. Low mentaIity but not complete helplessness.
10. Mental breakdown after maturity, especially from one of the major psychoses.
Sewall Wright, great statistician that he was, then graphed out these categories in this figure:
People in categories above the dashed midline contributed more to society than they cost, for people in categories close to the midline their cost/benefit was a wash, and people below the midline cost more than they contributed. In Wright’s view (and presumably the view of most of the genetics committee), anybody in Categories 7 or below cost more to society than they were worth. Oddly, those in Categories 5 and 6, were “acceptable” to Wright, even though their cost to society were greater than their contributions. He may have had a soft spot for playboy types, charlatans, and criminals, although he was also unsure of the genetic contribution to these traits .
Wright’s graph did not go unnoticed. Victor McKusick, whose obituary called him “The Father of Medical Genetics,” reproduced Wright’s graph in his 1964 short book Human Genetics, one of the earliest modern medical genetics texts. On page 141 of McKusick’s text, he goes on to say “No one would dispute the desirability and scientific soundness of encouraging reproduction of intelligent persons who are an asset to society.” And it didn’t end there. Cost effectiveness studies continued to be raised to justify the introduction of heterozygote carrier screening and amniocentesis in the 1970s and beyond.
From an ethical perspective, I find it appalling that the cost-savings to society is hailed as a benefit of expanded carrier screening. Do we really measure the worth of a human life by how much money they contribute or cost to society? Isn’t that whatpeople with disabilities, their supporters, their families, and disability scholars have been screaming at us for like a million years? Are we that tone deaf that we can’t hear their shouting? Are we just pretending to hear them or are we simply ignoring them? Isn’t a human being’s worth measured by non-economic factors? Who’s to say whose life is more worthwhile than others or how it should be measured? Why is it that people born with a genetic condition are less valued than people who develop disorders after birth that are even more economically burdensome, like dementia, lung cancer, diabetes, and heart disease (the risks for many of which can be reduced by low cost interventions like improving diet and exercise, and avoiding tobacco and excessive alcohol intake)?
Cost-savings justifications are also incompatible with Diversity, Equity, Inclusiveness, and Justice (DEIJ) initiatives. Money-saving justifications imply that if you are born with a genetic condition and cost society too much money, we are not going to include you. The message is that we support DEIJ for the “right” kind of people, those whose genomes and phenotypes aren’t too costly.
From a technical standpoint, many cost-effectiveness studies suffer from some serious flaws. For example, the Beauchamp et al. paper mentioned above includes 176 conditions in their analysis. Realistically, and which the authors acknowledge, there is no way to obtain reliable lifetime costs of all 176 conditions, given the rarity and variable prognosis of most of them. Also, the greatest economic cost benefit comes from the conditions associated with increased likelihood of survival to adulthood and the attendant need for ongoing care, such as Fabry disease, cystic fibrosis, the hemoglobin disorders, and Wilson disease. Adding on dozens and dozens of other uncommon conditions, often associated with early death, does not add much to the economic savings (a point also made in the paper by Azimi et al., cited above).
Cost-savings studies also often make the erroneous assumption that people who have a genetic condition make little or no economic contributions to society. Tell that to all the hard-working adults with Fabry disease, cystic fibrosis, deafness, hemoglobinopathies, etc. Not to mention the many non-economic benefits that any individual – regardless of their genome or phenotype – may “contribute” to society, such as joy, love, friendship, community, artistic creativity, etc.
But you might argue that health resources are limited and saving billions of dollars can’t be ignored, whatever the exact amount. That saved money could go to treating people with genetic conditions. Well, first off, there is no reason to believe that such abstractly saved money would be funneled directly into the care of patients with genetic conditions, or for that matter back into the health care system itself. The theoretically saved money could just as easily wind up funding some legislator’s pet project.
Furthermore, the savings are not quite as impressive as they sound. For arguments sake, let’s accept the estimates of Beauchamp et al. that on average each condition incurs a lifetime cost of $1.1 million (US) and that 290 of every 100,000 pregnancies are affected by one or more of these 176 conditions. Assuming about 3.6 million births in the US each year, that would result in 10,440 children with one of the screened conditions. At a lifetime cost of $1.1 million each, that adds up to ~$11.5 billion in savings over their lifespan (I am making a “best” case but unrealistic assumption that all at risk couples are identified and all affected births are avoided by preimplantation genetic testing, prenatal testing and termination, avoiding reproduction, gamete donation, etc. Cost-effectiveness studies of course don’t make such unrealistic assumptions).
On the other hand, the annual (not lifetime) spending on all health care in the US is $4.3 trillion, per the Center for Medicare & Medicaid Services. The lifetime costs of caring for people with the conditions included in an expanded carrier screening panel is barely a rounding error in annual health care spending in the US. Is the purported savings benefits of expanded carrier screening worth a rounding error, in light of its ethical shortcomings?
Figures 2a and 2b from the Beauchamp et al. reference cited above, illustrating the cost-effectiveness of different carrier screening strategies. Note how the graphs visually evoke the Sewall Wright graph above.
Another justification offered for ECS is the claim that money is saved by shortening the diagnostic odyssey and thus reducing visits to specialists and avoiding unnecessary and inappropriate treatment and testing. Certainly shortening the diagnostic odyssey is a laudable and important goal. However, cost calculations based on that claim are likely to be flawed. We don’t know how many babies born with the screened conditions would experience a diagnostic odyssey, how long the odyssey would take for each condition, and how much unnecessary spending would have been avoided. Nor do we really understand how many children undergo the diagnostic odyssey overall or what percentage of these journeys might be avoided by expanded carrier screening. Besides, the diagnostic odyssey could be more effectively shortened – though by no means eliminated – by expanding newborn screening and/or improving the availability of, and access to, whole genome sequencing, which would allow diagnosis of a much broader range of conditions than those included on carrier screening panels.
A potential and subtle danger of emphasizing the economic benefit of ECS lies in the absurd economics of healthcare that results in the high cost of new and innovative ways of treating genetic disease based on the underlying pathologic variant. Delandistrogene moxeparvovec-rokl (Elevidys), an anti-sense oligonucleotide (ASO) for approved by FDA in June for treating Duchenne muscular dystrophy patients with certain dystrophin variants, is priced at $3.2 million (US). As pointed out by Dan Meadows in this space a few weeks ago, the cost of nusinersen (Spinraza), another ASO, to treat some forms of spinal muscular atrophy, is estimated to cost ~$750,000 (US) the first year and $375,000 per year thereafter. Such high costs of treatment further bolster the belief that treating genetic disease is too costly. Paradoxically, just as at least partially successful treatments are finally becoming available for some genetic conditions, there may be a move to further prevent more births of people with certain genetic conditions in order to save money.
It’s tempting to equate cost-savings with eugenics. However, I think the eugenics label adds nothing to the discussion, other than being an accusation that turns the discussion into an argument. Whether or not it’s eugenic depends on how you define eugenics, and there is no widely agreed on definition. I think it is inaccurate to broadly label medical genetics and genetic counseling as modern day eugenics. Nonetheless, arguments for cost savings and disability prevention betrays the field’s eugenic roots and how we have not fully come to grips with our history. The graphs and table displayed in this post are not exactly the same, but they do share a pedigree. With each generation, the graphs and tables change to reflect their times, but the underlying message remains constant.
Medical geneticists and genetic counselors are not an unethical bunch. In fact, I have always been impressed with how much we struggle with complex ethical issues on a daily basis. But our vision can be subtly influenced by our history and by the fact that many – probably most – clinical and laboratory positions rely on the availability of genetic testing. We try to so hard to be good but sometimes it blinds us to the bad we might do. As Devin Shuman so elegantly reminded us in this space last week, the good intentions of our ableist assumptions can do a lot of harm. It’s about time we shed the ethical baggage of economic savings based on avoiding the birth of people with disabilities.
















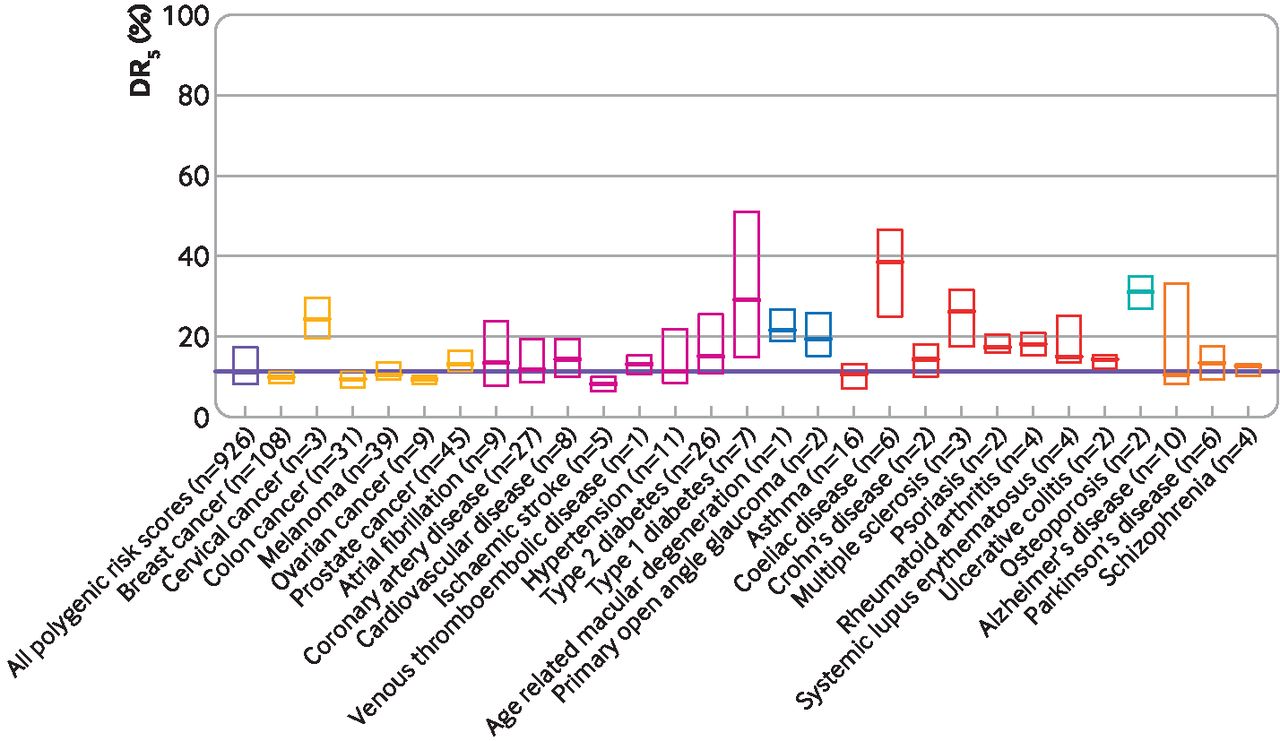
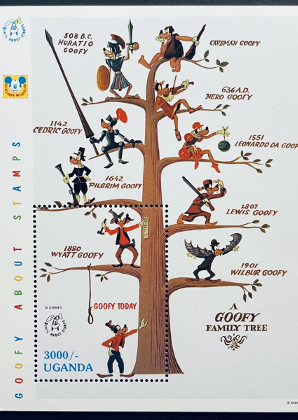


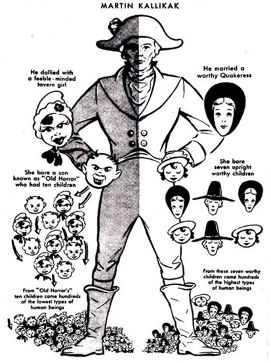
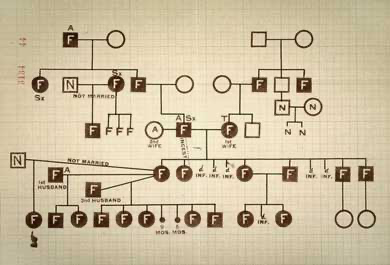




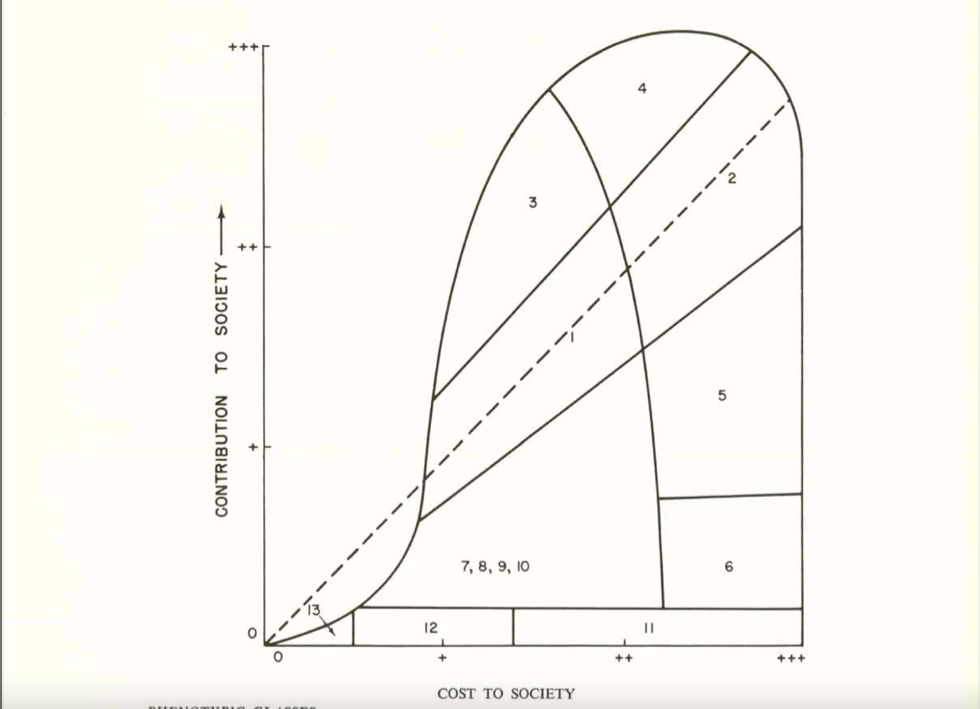


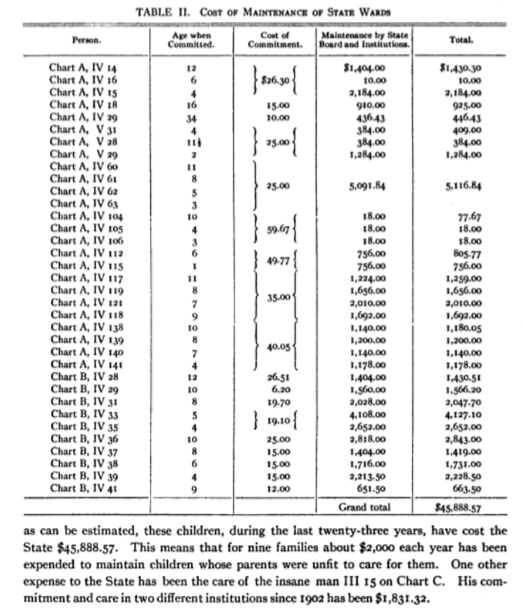

{kind=link}
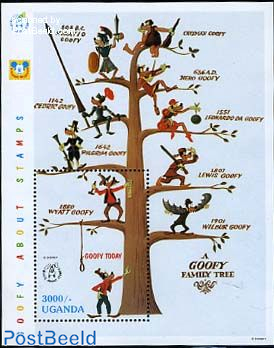{kind=link}