
In a recent thoughtful commentary in Genetics in Medicine and an ELSIhub Journal Club, Amicia Phillips, Maria Siermann, and colleagues critically examined the concept of actionability in the context of prenatal and newborn genomic screening. The authors conclude that actionability is poorly operationalized and call for “a need to develop a clear and nuanced understanding of actionability to ensure that screening policies are both ethical and effective.” I am not going to re-hash their ideas here, but some key considerations they raise include asking the questions Actionable how? Actionable when? Actionable for whom? Actionable at what level? I encourage you to read the article and view the ELSIhub Journal Club when the recording becomes available.
I have no insights or suggestions on how to develop a better understanding of actionability. I will leave that to folks smarter and more informed than me. But the article and webinar got me to thinking about the relationship between utility and actionability. Here I propose a model for thinking about these concepts and how they might be applied in genomic medicine. I recognize that both concepts are plagued by ambiguity. But for purposes of my model, utility is defined as the likelihood that a genomic/genetic test will, by prompting an intervention or other action, result in an improved outcome (a slight modification of the NCI definition). Going with the Phillips et al. paper, actionability is defined as “whether the information generated by screening leads to actions that may be undertaken” (to which I would add information generated by diagnostic testing too).
Utility typically includes two domains – Personal and Clinical Utility. In my model, I include a third domain that I call Public Health Utility. The types of actionability vary within each domain.
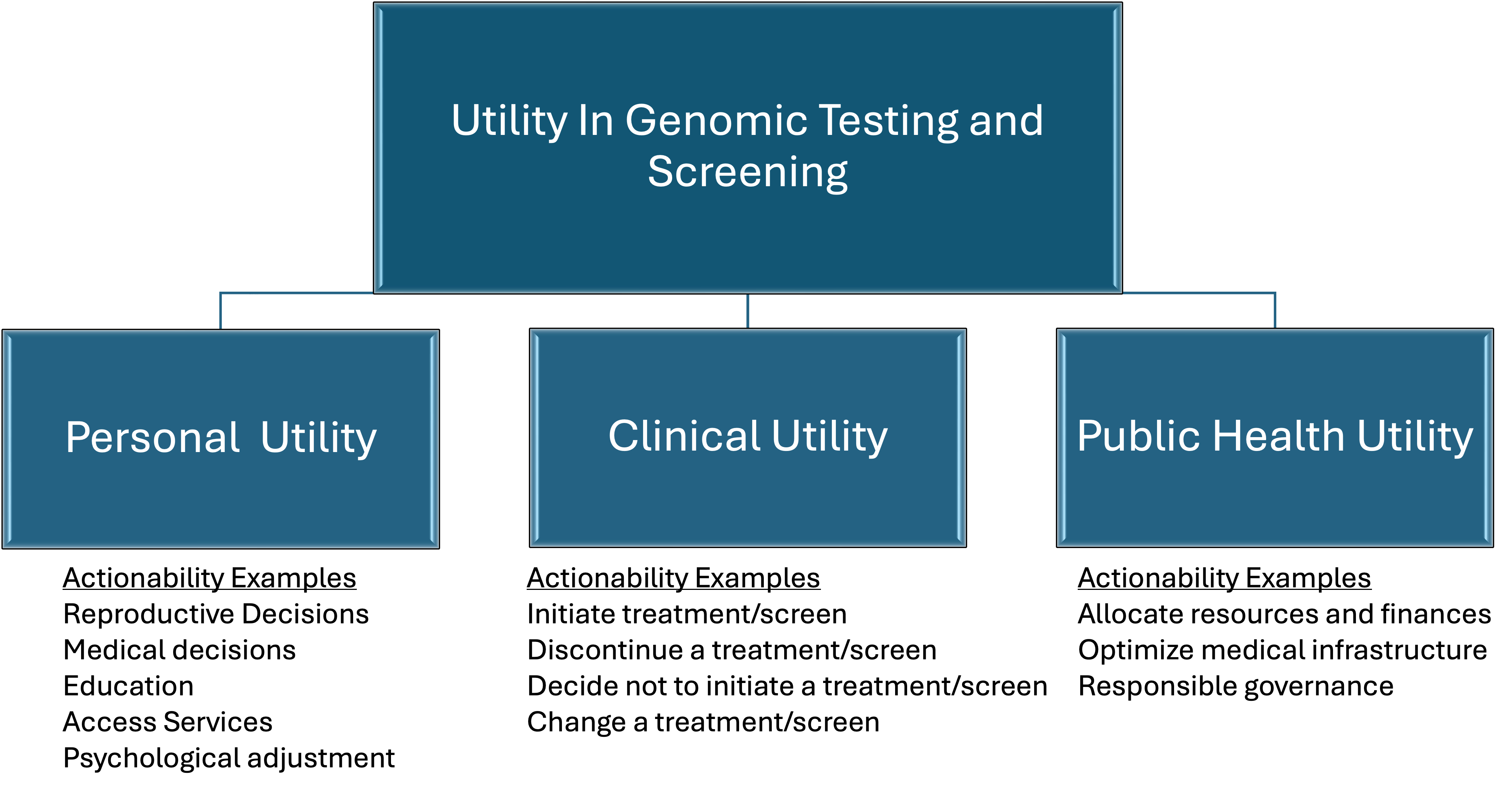
Personal Utility can be measured by the efficacy of actions that a person or family may take as a result of genomic/genetic testing that has the potential to improve their emotional, psychological, medical, and socioeconomic well-being. Using the recommendations of Kohler et al., these can be broadly categorized as affective, cognitive, behavioral, and social benefits. Some examples of actionability items include making reproductive decisions; choosing (or not) a medical course of action; joining a support group; accessing educational resources such as an appropriate educational plan for a child; applying for health and financial benefits such as Medicare and Social Security Disability Insurance in the US; participating in research about a specific genetic condition; and engaging in a psychotherapeutic relationship and other measures that can enhance emotional and psychological adaptation to a test result or genetic condition in the patient or within a family.
Clinical Utility can be assessed by the efficacy of actions that a clinician may take as a result of genomic/genetic testing that could improve the health outcomes of a particular patient or set of patients. These might include instituting specific screening modalities such as medical imaging as well as pharmaceutical, surgical, and other treatment and risk-reducing strategies, or suggesting alternative strategies. Actionability can also paradoxically include non-actions, such as discontinuing a treatment or recommending against a treatment or screening modality.
Public Health Utility can be assessed by the efficacy of actions taken by governmental and professional bodies based on genomic/genetic testing that may improve health outcomes on a population level. These actions might include allocating resources and finances, optimizing medical infrastructure, identifying research priorities, establishing clinical guidelines, and ensuring socially just and equitable access to genetic testing and subsequent recommended medical care and other health-related resources.
All three domains of utility feed into one another and are intertwined like a triple helix, so it can be difficult sometimes to separate them out. But the model* does provide a framework for evaluating utility and actionability. A test can be evaluated for its actionability in the different domains and weighed for the benefits and risks across domains. A test might provide little Clinical or Public Health Utility but still be justified if it provides significant Personal Utility. Or within a given domain, actionability may not provide enough utility to justify the test but if the benefit is moderate across all 3 domains the sum of the benefits may provide enough utility to justify the test. Or a test may have different actionability at different times of life and that too can be included in assessing utility.
Decisions about the utility of the actionability of genomic/genetic testing should be based on ethics, resource and financial availability, practicality, and statistical analysis, with input from patients, clinicians, the public, researchers, health policy analysts, and other stakeholders. Phillips et al. offer a much needed nudge in that direction. Of course, what counts as a benefit and how to weigh those benefits is no simple matter but that should not stop us from going through the process. Fear of imperfection should not be the enemy of the good.
Artificial Intelligence was not used to research or compose or edit this blogpost, nor was it used to generate the image.
_________________________________________________
- Okay, let’s call it The Resta Model or The Resta Framework. Unless somebody else has already proposed this model and I didn’t realize it or it turns out be be a lousy model in the real world.
