In this post, the word “fat” is used intentionally to follow the language of fat advocacy organizations. This is meant to challenge the notion that the word “fat” is inherently bad but rather is a neutral descriptor that describes the bodies of many people. As with other identities, individuals may prefer the use of other terms to describe themselves, in which case it is always best to mirror that language.
Genetics is at the core of many efforts to address the “obesity epidemic.” Genetic tools such as polygenic scores, CRISPR-Cas9 technology, and direct-to-consumer genetic tests share the goal of minimizing fatness. Not only do these efforts ignore the already understood social determinants related to weight and health, but they consistently exclude the perspectives of fat people. Additionally, gene panels designed to identify monogenic causes of obesity raise concerns; while they might be able to provide actionable medical information, the focus should not be exclusively on weight loss.
When we center weight loss as the main mechanism to support one’s health, we reinforce the persistent idea that if someone is fat, they are, by definition, unhealthy, and addressing their weight, therefore, must be a top priority. This can lead to experiences where people’s health concerns are not taken seriously or further explored, perpetuating mistrust in the healthcare system and subpar care. As the genetic counseling profession strives to promote more inclusive and equitable spaces, it is important for us all to reflect on our own biases and minimize over-pathologizing fatness.
Anti-fat bias is pervasive
Fatness is unique in that it is both externally visible and it remains socially acceptable to point out or express dislike for. One’s weight is often attributed to a direct depiction of a person’s character or behavior. Fat people are seen as “lazy” and “lacking willpower,” while thin people are perceived as having “earned” their societal advantage. In her book Hunger, Roxane Gay writes,
“When you’re overweight, your body becomes a matter of public record in many respects. Your body is constantly and prominently on display. People project assumed narratives onto your body and are not at all interested in the truth of your body, whatever that truth might be. Fat, much like skin color, is something you cannot hide, no matter how dark the clothing you wear, or how diligently you avoid horizontal stripes” (page 31).
Media reinforces these beliefs. Popular films and TV shows such as Super Size Me and The Biggest Loser present opportunities for viewers to pass judgment on those who engage in “fattening behaviors” while further solidifying one’s pre-existing belief that thinness is earned by a series of correct decisions. Even in the recently released Wonka, fatness stemming from gluttony, selfishness, and poor morals is used repeatedly as a punchline. News coverage of the so-called “obesity epidemic” is filled with unflattering images of “headless” individuals, often sedentary or eating “unhealthy” food. Imagery such as this works to remove the humanity of people who are fat and further the widespread belief that fatness is simply a result of “bad choices.”
Similar to other forms of oppression, people experience anti-fat bias in many ways. For example, there currently exists no federal protections and very few state protections against weight-related discrimination in the workplace. Fat people are often the subject of undesired critiques of their bodies, typically said under the guise of “caring about their health.” No space may be more dangerous for fat individuals than healthcare, where weight is weaponized against patients by providers claiming to “do no harm.”
While the relationship between health and weight is tenuous, there is a clear relationship between anti-fat bias and adverse health outcomes, including increased stress levels and healthcare avoidance. When individuals seek care, the quality of care they receive is often lower. For example, when seeking cancer screening as a person who is fat, there are many barriers, including providers who will deny services such as a Pap smear based on weight. Additionally, there is a history of the medical system causing harm through the over-prioritization of weight loss. One such example is that of Fen-Phen, a combination weight-loss pill that was eventually recalled due to it causing valvular heart disease.
Increasing accessibility to genetic counseling for patients who are fat
Genetic counselors provide support for individuals navigating healthcare spaces. Even though someone’s weight is not the indication for an appointment, people who are fat do not come to us in a vacuum. Rather, we fit into their broader experience seeking healthcare, which often includes experiences of bias and stigmatization. We must understand these experiences to provide adequate support and mitigate additional harm.
Genetic counselors must examine how to make their practices more inclusive for fat people. Are the chairs narrow and with arms, which may be uncomfortable for someone who is fat? Is there utility in taking the weight of the patients you see for your appointment? How is weight used in cancer risk assessment models? Are you making assumptions about someone’s health-promoting behaviors based on their weight? How do you discuss healthy diet and exercise? How are you discussing and recording no-call cfDNA results, challenges with ultrasonography, or limitations of standard MRIs being able to accommodate some people’s body size?
We also must be mindful of our language. For many fat people, the common-in-healthcare descriptor of “obesity” often evokes a negative response and feels overly medicalized. The term obesity is also a direct reference to the Body Mass Index (BMI), an ineffective predictor of health with racist origins and uses. Similarly, avoiding the use of phrases such as “struggling with their weight” to describe people can help mitigate the idea that being fat is inherently something one struggles with.
For decades now, fears of the “obesity epidemic” have harmfully implied that a person’s fatness is inherently detrimental to society at large. Over time, these ideas become so ubiquitous that people rarely question them. As genetic counselors dedicated to providing unbiased and supportive care to all of our patients, we need to understand the importance of unlearning and reflecting on systems of oppression, and anti-fat bias must not be an exception.
Sarah Wiser, B.S. (she/her) is a second-year genetic counseling student at Boston University Chobanian & Avedisian School of Medicine. Sarah is passionate about promoting equitable access to genetic counseling services and challenging anti-fat bias in healthcare.
This spring we will welcome a record number of new genetic counselors to the field. Based on 2022 year Match data from the National Matching Service Inc, we expect >500 new graduates in 2024.* The growing number of graduates is the natural result of more training programs and expanding class sizes in existing programs.
Unfortunately, it seems that this record number of new grads arrive to one of the worst job markets for genetic counselors in many years. Based on conversations I have had with a number of recent or soon-to-be genetic counseling graduates and informal conversations with several genetic counselors involved with training program administration, many new grads are having a hard time finding that first position. It is really tough for job seekers right now.
I am writing this to provide some historical background about why we might be in this position, and where we have so missed the mark in terms of supply and demand. It is my hope that we can learn from these mistakes and make changes as a profession to improve job opportunities, growth and security while also improving genetic services.
I am also writing though because I want to give assurance to all those entering the field in 2024 that it will get better. When I graduated, 20+ years ago I came out of my training program without a job, and I know how devastating and heavy that can feel. The job market has waxed and waned in the past and the pendulum will swing the other way at some point. The reason for my optimism is that, although our current job boards don’t reflect this, I believe that now, more than ever there is a need for the expertise and services that we can provide as genetic counselors. I want to reassure you that you will one day find that perfect job. And I also want you to know that the fact that you don’t yet have a job yet is not your fault.
How did we get here?
Recent history provides context for how we got to this point. Just over a decade ago, three major events rocked the field of clinical genetics:
Although it is hard to believe that there was a time before next generation sequencing (NGS), Sanger sequencing was the standard for many years. NGS allowed for gene sequencing to be done more cost-effectively and around 2010 we started seeing more multigene panels come to the market.
In late 2011 the first prenatal cell-free fetal DNA screening test, MaterniT21, became commercially available through Sequenom. In the years that followed, versions of cfDNA tests were released by multiple companies, creating an intensely competitive commercial landscape.
In June of 2013, Myriad Genetics lost their monopoly on BRCA1 and BRCA2 testing when the U.S. Supreme Court ruled that human genes could not be patented in the landmark case, Association for Molecular Pathology v. Myriad Genetics. This opened an opportunity for many labs to enter the genetic testing market.
All of these factors contributed to an enormous growth of the genetic testing industry and rapid escalation in demand for genetic counselors. The commercialization of the field of genetic testing was unlike anything we had seen before. Genetic testing was front page news and investors were lining up to be a part of it. Labs, flush with venture capital money, created many new job opportunities for genetic counselors.
In some cases, the job creation was very direct, with labs hiring genetic counselors as medical science liaisons, or to work in variant interpretation, product development and direct patient care roles. In other cases, the jobs created were with the telehealth companies labs hired to provide genetic counseling support to providers and patients ordering their brand of test. Additionally, the growing availability of genetic testing and investment in genetic testing technology created jobs in hospitals, clinics and research settings.
By 2015 it was clear that the demand for genetic counselors exceeded the number of trained people to fill the jobs. The following data was presented at the National Society of Genetic Counselors Annual Conference in 2015:
This graph contrasted the number of job postings on the NSGC job board with the number of genetic counselors coming out of training programs. In 2015, we had 291 genetic counseling program graduates compared to 655 job postings.
I am sad to say that this year, with ~500 graduates, there are 44 jobs listed on the NSGC job board at the time of this writing, and about half of these are not listings for genetic counselor jobs. In part, this reflects the fact that companies are not using the NSGC job board as their one and only means of recruitment, but it is also, undeniably, an indication that there are not many open jobs right now.
In 2015, a Workforce Working Group (WFWG) was established comprised of representatives from the American Board of Genetic Counseling (ABGC), the Accreditation Council for Genetic Counseling (ACGC), the Association of Genetic Counseling Program Directors (AGCPD) and the National Society of Genetic Counselors (NSGC). The charges to the WFWG were as follows:
● Identify current and future barriers and opportunities that impact the growth of the CGC workforce.
● Make recommendations to and support the development of specific action items that will facilitate growth of the profession and minimize and/or remove barriers to expansion.
● Drive and coordinate the efforts of the professional genetic counseling organizations to ensure the action items recommended by the working group are carried out in the most efficient and effective manner possible.
The WFWG commissioned a consulting firm, Dobson DaVanzo & Associates, LLC, to conduct a workforce supply and demand projection study of certified genetic counselors in the US over the time period from 2017-2026. This report considered many factors as they attempted to project the future needs and factors that could complicate their estimations.
The report developed two models in which the projected need for genetic counselors was 1 per 100K or 1 per 75K population and they projected we would reach equilibrium for the 1 per 100K model by 2026. While the workforce study recommended expanding existing training programs and developing new programs, they warned, “activities around this initiative will be focused on accelerating growth, while being mindful of not overreaching and exceeding demand.”
The report also raised concern regarding a “substitution effect” which was defined as other healthcare providers providing genetic counseling to patients. Additionally, the Dobson DaVanzo report also cautioned, “policies that restrict reimbursement to direct patient care by certified genetic counselors who are not affiliated with a commercial laboratory would likely reduce the effective demand for care, while at the same time reducing the ability of providers to meet patient need.”
This workforce report provided guidance on the importance of cautious growth with the caveat that it was an uncertain and rapidly changing landscape. The current situation has left me questioning if our profession considered this report in full as we have grown our workforce?
We met the Dobson & DaVanzo report’s projection of ~6.5K certified genetic counselors in March of 2023, more than 3 years ahead of schedule, and we continue to have more genetic counselors graduating from training programs than ever before. It does not appear to me that we have been “mindful of not overreaching and exceeding demand.” Of the 55 programs listed on the ACGC website, 14 are designated “new accredited programs”, and there are an additional 6 applications for programs in the works.
The substitution effect was defined by Dobson & DaVanzo as non-genetic counselors doing genetic counselors’ work. For the most part, we have not seen nurse practitioners, physician’s assistants or other providers stepping in to do the work of genetic counselors. From my view, what we have seen is that we are increasingly substituting ourselves. Let me explain. The labs understand that to compete in this market, it is essential to package genetic counseling with genetic testing. I see the labs going to providers who are neither equipped to nor interested in doing the counseling themselves, and offering complimentary genetic counseling as a perk for those ordering their brand of testing. The problem is, in many cases, genetic counseling provided gratis by a laboratory is not comparable to what would have been provided by a non-lab-affiliated genetic counselor in a clinical setting. The patient may get a message through a portal that tells them they can schedule a genetic counseling appointment. They may talk with a genetic counselor by phone for a few minutes to review results. What they rarely receive in these encounters is the comprehensive genetic counseling care that was factored into this workforce study. At this point, many providers and patients believe that this test-bundled follow-up care is standard genetic counseling. And, used to getting it for free, many providers and healthcare systems are now unwilling to pay what it costs to have genetic counselors on staff.
As important as it is, our profession has largely ignored the issue of how we are paid. This not only affects our job prospects, it affects the level of care we are able to offer to our patients.
The genetic testing lab bubble that began around 2013 created jobs funded by easy access to business loans and venture capital. Labs could use their huge investor funds to pay nice salaries to genetic counselors even when their companies were losing millions (and in many cases, hundreds of millions of dollars a year). The workforce study was developed at the time of this bubble and did not take into account the possibility that this job creation was unsustainable. Now, the VC bubble is deflating. After a decade of sustained and significant losses, investors are no longer willing to keep these labs going without return on their investment. Borrowing money has also become increasingly expensive and difficult. As a result, we are seeing labs retrench, close or be absorbed by competitors, with resultant layoffs of genetic counselors. And with many in our field looking for work, we have yet to reckon with the fact that we still don’t have a viable and sustainable funding model for genetic counseling services – in large part because fair reimbursement is difficult to demand when some version of genetic counseling services have so often been given away for free.
Another bit of history, and one the WFWG could not have factored in, was a global pandemic. Undoubtedly COVID-19 disrupted healthcare in ways that affected genetic counselors. As to the big picture, I think one important issue connected to the pandemic has been some of the financial challenges faced by many industries. For example the interest rate hikes, which have been a tool used to try to curb inflation has made funding more expensive and difficult to secure. The timing of this is unfortunate given the recent position of the labs. However, this does not change the fact that growing a profession on the basis of borrowed funds and start-up investors put us in a precarious place even without the added financial challenges brought on by the pandemic.
What comes next?
Given all that has changed over the last decade, and because we are nearly at the end of the period that the Dobson DaVanzo study had projected, I hope the WFWG has plans for another workforce study. Our profession is in need of an updated analysis of workforce issues.
Until we find a way to fund genetic counseling positions that does not rely on the house of cards that is laboratory funding, we should be mindful that our program growth does not outstrip the job opportunities for our newest colleagues.
The rapid growth in training programs suggests that the institutions involved looked at the rosy growth projections and ignored the recommendation to proceed with caution. Between the challenging job market and the difficulty securing clinical training sites for students, I imagine many involved in training programs are alarmed. While we have added many training slots, the program I attended, at Brandeis University, closed at the end of 2022 because there weren’t enough clinical training sites to serve the number of enrolled students the school required to cover the costs of maintaining the program. More programs may soon be facing tough decisions like this. One program director I spoke with shared, “many programs do not receive any state funding which means they have to run completely on tuition dollars. Even one student difference can break a budget that relies on those tuition dollars and may result in a program closing.”
In addition to considering carefully the growth of our profession through the training programs it is imperative that we all continue to advocate for fair reimbursement. The work we do as genetic counselors is valuable and crucial to the ethical practice of genetic healthcare, now more than ever. And I expect the need will only grow from here. But, we risk not being able to be in these roles, providing care and expert guidance if we do not first ensure that we have sustainable reimbursement for our services. Every single one of us needs to advocate for the “The Access to Genetic Counselor Services Act” so that genetic counselors are recognized by Medicare and can be reimbursed for the services we provide. This is everything. Have you contacted yourrepresentative?
I also hope we can mobilize as a profession to advocate for comprehensive standards of care in our work as genetic counselors. We should reflect on the recent challenges and disruptions we have seen in the field and consider how we are defining the practice of genetic counseling. If we continue to allow the profit motives of the labs to push us to act more as genetic testing facilitators, we will have an increasingly difficult time sustaining our ability to provide comprehensive genetic counseling and support.
Lastly I would like to send a message to all of the new and soon to be graduates who do not yet have jobs secured. Please don’t lose hope. You are the future of our profession, and we need you to help move us and genetic services forward for the better.
*The original version of this article stated, “A report published in 2022 by the Accreditation Council for Genetic Counseling (ACGC) indicates that ~800 genetic counselors will complete their training at the 55 accredited training programs.” and referenced the following report: https://www.gceducation.org/wp-content/uploads/2023/06/ACGC_2022_AnnualReport.pdf This was changed to reflect data from the National Matching Services Inc statistics, which reported that 547 applicants matched with a GC program in 2022.
A guest post by Ambreen Khan and Kimberly Zayhowski
Normative standards of professionalism dictate that a professional should remain apolitical, positing that separating personal beliefs from professional endeavors allows one to maintain objectivity. The enforcement of these standards is increasingly evident in genetic counseling spaces, such as with censorship in workplace meetings, on discussion forums and social media, and at conferences.
However, remaining apolitical grows complex given the politicization of everyone’s identities and personhood. The intertwining of personal, political, and professional realms is undeniable, often operating subconsciously. Operating in a makeshift bubble of neutrality disconnects us from the lived realities of our colleagues and the patients we strive to serve.
Eugenics underpinnings in genetic counseling
The roots of the genetic counseling profession are entangled with a history steeped in eugenics, a movement advocating for selective breeding to enhance the human population by using erroneous assumptions about genetics shaped primarily by social, political and personal biases of its supporters. Originating in the late 19th century, eugenics principles guided the atrocities committed during Nazi Germany’s reign, heavily shaped by American eugenicists like Charles Davenport and studies from the Eugenics Record Office at Cold Spring Harbor Laboratory. The historical justification of eugenics to forcibly sterilize, criminalize, and perpetrate genocide against minoritized communities has been rooted in the misappropriation of genetic and medical concepts. Therefore, dismissing the importance of politics in the field of genetics is a fallacy.
Genetic counseling’s origins can be traced back to the ethically fraught ideology of breeding out those considered less “desirable.” The justification for establishing and funding the first genetic counseling program suggested that genetic counseling serves as a strategy to mitigate hereditary diseases and encourage individuals to make informed decisions regarding reproduction, both for their own well-being and that of the broader population.
Despite the prevailing belief among genetic counselors that we are staunchly anti-eugenics, traces of eugenic ideology persist within certain aspects of our practice, aligning with broader political and power structures. This is exemplified by the recent NSGC Practice Guidelines suggesting the use of expanded carrier screenings as a means for downstream cost-savings through the prevention of births of individuals with certain genetic conditions.
Moreover, genetic counselors’ desire for absolute neutrality ties closely with the need to adopt a non-directive approach with patients, obscuring the intrinsically directive nature of everything said and done in patient interactions. This connectioncan be traced back to post-WWII geneticists’ efforts to distance themselves from eugenics, despite perpetuating comparable ideologies under the guise of neutrality. The norm to remain apolitical perpetuates self-censorship, impeding the field’s ability to openly confront its connections with eugenics.
The impossibility of neutrality
Acknowledging personal political beliefs becomes a crucial aspect of a genetic counselor’s professional journey and our interactions with colleagues. As Lewis Wallace, a transgender reporter, asserts in his piece titled “Objectivity Is Dead And I’m Okay With It,” neutrality is not real, particularly for people with marginalized identities who cannot remain neutral or centrist in debates concerning their own humanity. Hence, the structures demanding neutrality in the face of oppression must be challenged.
Numerous contemporary policies, such as those regarding immigration, disability and reproductive rights, racial justice, education, LGBTQIA+ rights, colonialism, imperialism, and more, directly impact how we show up in our professional lives. Policies can impede our capacity to pursue a career, such as when they impact visa status, restrict access to safe and inclusive work environments, or perpetuate discriminatory practices such as anti-transgender legislation.
The politicization of religious and ethnic identities to justify violence exposes individuals to bigotry, threatening their safety and sense of belonging. Politics can profoundly affect mental and physical well-being, as evidenced by US-funded genocide in Gaza and settler colonial violence in the occupied West Bank, leading to distress and safety concerns among Palestinian genetic counselors as well as allies that speak out against these atrocities. In such instances, neutrality serves oppressors, demanding marginalized individuals to suppress their emotions and well-being to conform to “professionalism” standards, which expect silence amid oppression.
The burden of representation and palatability
Standards of professionalism carry oppressive ideologies favoring white supremacy. Professionalism traditionally reflects the cultural norms, behaviors, and traits of the dominant social group, often represented by straight, cisgender, non-disabled white men in the broader field of medicine in the US, or women in genetic counseling. Consequently, professionalism tends to be assessed primarily among those who are racially minoritized, queer, gender-diverse, and disabled. An expectation of professionalism entails the ability to collaborate with others – even if those people say and do awful things. This creates an environment of dealing with microaggressions and discrimination quietly and laying low when witnessing bigoted conversations.
In navigating political dynamics, genetic counselors often encounter challenges with colleagues tied to respectability politics, a phenomenon where individuals from marginalized groups feel compelled to conform to mainstream expectations to gain social acceptance. Additionally, the pitfalls of “whataboutisms” arise, deflecting from the core issues at hand by pointing to separate problems or situations. This tactic often undermines meaningful discussions about systemic problems, diverting attention from the pressing need for change.
The pursuit of “palatability” within diversity, equity, and inclusion work can paradoxically prioritize the comfort of the oppressor over meaningful progress. Efforts to make conversations or initiatives more palatable risk diluting the urgency and discomfort inherent in addressing systemic issues. Individuals with minoritized identities often find themselves assuming the role of ambassadors for their communities. As they navigate professional spaces, they become de facto representatives, sharing the responsibility of dispelling stereotypes and fostering understanding. This burden is a consequence of existing in spaces where diversity is limited.
Integrating our personal, political, and professional selves
True progress in social justice work demands confronting challenging truths, dismantling entrenched power structures, and prioritizing the voices of marginalized communities over the comfort of those with privilege. Achieving this necessitates a deep understanding of one’s own privileges through an intersectional lens.
Without reflecting on the underlying reasons that necessitate our need to maintain objectivity while upholding the status quo, genetic counselors jeopardize their ability to engage in nuanced conversations with colleagues and patients. Staying engaged in global affairs is essential for genetic counselors to confront their personal biases and improve patient care.
Trusting ourselves and our colleagues to bring their authentic, political selves to professional spaces promotes meaningful dialogue and mutual understanding. The myth of apolitical neutrality acts as a barrier to recognizing the complexity of human experiences among colleagues and within ourselves. As we navigate the paradox of remaining apolitical in a world where identities are inherently political, genetic counselors must consistently question the root cause of their need for neutrality.
The opinions expressed in this article are solely our own and do not reflect the views and opinions of our employers.
Authors:
*Ambreen Khan, MS, CGC (she/her) works as a laboratory genetic counselor and a grassroots community organizer. A bilingual Muslim individual of Pakistani descent, Ambreen follows her passion of increasing access to equitable genetic services locally and globally, through educational talks, social media content, and research.
*Kimberly Zayhowski, MS, CGC (she/her) works as an assistant professor and research genetic counselor. A queer and multiracial individual, Kim is dedicated to advocating against oppression in genetic counseling research, education, and practice.
*Names in alphabetical order. These authors have contributed equally to this work.
In his poem American Sonnet Billy Collins compares a sonnet to “furrows in a small, carefully plowed field.” Classical sonnets are tidily structured works that more or less follow a format of 14 lines, often in rhyme, the last two of which offer a resolution to the problem or question set forth in the earlier lines.* The strictures and structure of a sonnet and the image of a plowed and furrowed field makes me think of how genetic counselors try to neatly organize genetic counseling sessions. The templated counseling notes we produce afterwards – some version of Patient Identification, Medical History, Family History, Counseling Provided, Summary and Recommendations – reinforce the idea of a structured session as well as the sonnet metaphor.
We try to impose structure, for reasons both good and not so good. In many clinical positions, most patients are coming to us with a handful of similar indications such that we wind up saying more or less the same things over and over, especially when we carry large patient loads. My roteness would become clear to me when a patient “interrupted” me with a question about something else altogether and I would forget where I was in my game plan. I was not listening to the message the patient was sending – they were not much interested in what I was talking about and they wanted to discuss something more important to them. Genetic counselors, with our professional insecurities, also subconsciously want to impress others with our arcane knowledge and prove that we can make an important contribution to the health and medical care of patients and their families. This manifests itself most acutely during the early stages of a career, when we are still slightly unsure of ourselves and are trying to establish a firm professional footing and reputation. But even wise veterans can get caught up in this style, including and particularly me (well, not anymore, now that I’ve converted to my favorite religion – Reitrementism).
While acknowledging the important role that numbers and information play in genetic counseling and patient care, a counseling session is at its core a psychological interaction between human beings. It took me – no kidding – a couple thousand counseling sessions before I even started to become a good genetic counselor and adapted my counseling to the basic psychological truth that the human mind usually expresses its emotional self in a non-linear manner. I knew this on a cognitive level but it took me years to actually incorporate this insight into my practice. To paraphrase Maya Angelou, people won’t remember what you said but they will never forget how you made them feel.
What does this mean in actual genetic counseling practice? I’m not advocating for omitting facts and figures or abandoning an over-arching loose structure. A counseling session should have a beginning and ending, and complex biomedical information often needs to be imparted. You can start out with a highly flexible plan of issues and information you think should be covered while at the same time be very willing to modify the plan or abandon it altogether to meet the unique needs of each patient. It might begin with a query as to what the patient wants to get out of the session, though some patients are better at articulating that than others and some just aren’t sure of what they want. But however you start, you need to be prepared for traveling with the patient as they veer off in often unclear directions that are sometimes different than what the patient originally articulated. Structure, numbers, information – they are so comforting and comfortable to us, like Collins’ neatly furrowed fields. But the safe zone of an organized educational format can make us hesitant to explore the unplowed fields of the patient’s psyche.
What we can discover in those unfurrowed fields is what is important to patients, why it is important, and how it influences the way patients makes sense of complex biomedical information and what they should do with it. Fear of going through treatment for cancer after having watched their parent’s body ravaged by chemotherapy. Anger at an employer for creating an emotionally or physically toxic workspace and attributing their cardiomyopathy to this environment. A deep belief in “natural cures” that is being challenged by their lack of efficacy in treating their child’s illness. Feelings of abandonment and resentment toward a parent who died when the patient was an adolescent and who is now a parent of an adolescent themselves. Fear of having a child with a disability. A marriage adrift on two different seas. Distrust of medical practitioners stemming from having been treated disrespectfully in past encounters. All of the technical information can be so damn scary they don’t want to talk about recurrence risks or the chances of getting cancer or variants of uncertain significance, at least not right away and not by listening to what sound like a verbal spreadsheet. Genetic counseling is supposed to make the patient feel emotionally safe, not the counselor.
What this requires is actually attending to what the patient is saying or asking, especially if it has little to do with what you are discussing. You don’t want to briefly comment on what sounds like a non-sequitur from the patient and then return to the safety of your comfortable structure. Following the patient’s lead can result in a session which travels in several different seemingly unconnected directions (Why is the patient going off at this angle?), loops back on itself several times (Hmm, why does the patient keep coming back to that?), or has you probing the patient with questions neither of you had anticipated (“And so you’re saying MRIs are scary to you because you have claustrophobia and you’ve also read that the MRI’s magnetic field is thousands of times stronger than the earth’s magnetic field at its surface, and that’s why you are reluctant to undergo hereditary cancer testing?”). It can become a near stream of consciousness session that resembles James Joyce’s Ulysses more than Elizabeth Barrett Browning’s tenderly romantic How Do I Love Thee?. Joyce’s novel begins with the famous opening line that seems to presage a typical narrative – “Stately, plump Buck Mulligan came from the stairhead, bearing a bowl of lather on which a mirror and a razor lay crossed.” – then quickly changes tone and explores the depths of the minds of the novel’s characters and ends with Molly Bloom pouring out her innermost thoughts in an unpunctuated iambic-pentameter-be-damned eight sentence ~22,000 word uninhibited and unfiltered soliloquy. Kinda’ like a counseling session can go (Nothing against Barrett Browning. She is a marvelous poet; just a different style than Joyce’s).
I don’t know how AI chatbots will play out in the genetic counseling arena and how they might influence the structure of genetic counseling sessions. It seems possible that they might one day be capable of carrying out a psychologically sophisticated interaction with a patient that matches a counselor’s skill set as well as taking into account the patient’s socioeconomic situation, though I suspect not in the immediate future and hopefully not until the ethical issues have been addressed (for an amusing take on chatbots and genetic counselors, check out my post Genetic Counselor Reinvented). My bigger immediate concern is that administrators will simply see chatbots as a replacement for genetic counselors rather than as an ancillary tool for genetic counseling. Or that administrators will employ a strategy that employs both genetic counselors and chatbots but increases counselors’ patient loads on the premises that chatbots are doing a lot of the work and so you can fit more sessions into a counselor’s schedule. This ignores the emotional toll on genetic counselors who work with patients in stressful situations and will likely lead to counselor burnout and poorer quality patient care.
The potential and concerns about AI aside for now, the semi-chaotic session is often more valuable to patients than the biomedical lecture. Yeah, it can look and sound like a mess and be just as dense and difficult to understand as Ulysses. But that mess is where the beauty of the patient’s mind lies. Which is why we need to use our counseling skills to sort through the mess and understand the psychological meaning of the patient’s words, beliefs, actions, and choices. Hence the wonderful messiness of genetic counseling.
The Brain — is wider than the Sky — For — put them side by side — The one the other will contain With ease — and You — beside — by Emily Dickinson
Over the centuries, poets have played with the format of the sonnet to breathe new life into it, such as Wanda Coleman’s American Sonnet 91 and other of her decidedly non-linear poems that explore race and racism in America.
At the recent annual conference for the National Society of Genetic Counselors (NSGC) in Chicago, there was a spirited debate about whether or not to change the genetic counselor name. An alternate name was not presented, but below is a word cloud of proposed alternate names which DNA Exchange author Bob Resta shared in his recent blog post, where he decided to decline supporting a name change.
An informal poll that was circulated after the debate found that a significant percentage of genetic counselors were also wary of pursuing a name change.
For those who have not seen the debate, there were two primary tensions between the “pro change” side and the “pro same” side. The “pro change” side argued that changing our profession’s name could bolster NSGCs Justice, Equity, Diversity and Inclusion (J.E.D.I.) action plan (https://www.nsgc.org/JEDI), theorizing that possibly one of the reasons that genetic counseling is less diverse than many other professions is that our name creates a branding and recruitment problem. The “pro same” side brought up that if we genetic counselors change our name, then we’d need to update all of our state licenses, plus the language in our pending legislation to have Medicare recognize genetic counselors. Mr. Resta agreed that these issues were also an important factor to consider. The pro-same side also brought up that Physician Assistants are currently changing their name to Physician Associate, and that the associated cost of their name change is estimated at approximately $22 million, which would obviously be a staggering expenditure for an organization like NSGC.
Looking further at the “pro change” perspective, NSGC has rightly committed itself to implementing a successful J.E.D.I. Action Plan. Diverse teams provide better clinical care, better research, and build better businesses, all sectors where genetic counselors commonly contribute. Competing for diverse talent is in many ways the competition for the future. In a white paper published by the consultancy McKinsey in 2020, titled “Diversity Wins: How Inclusion Matters,” they outline the many ways that more gender and racially diverse organizations consistently outperform their less diverse competition, and argue for a greater focus on multivariate diversity (meaning “going beyond gender and ethnicity”). Currently, genetic counseling is among the least ethnically diverse fields in healthcare. We genetic counselors have an enormous amount to gain from a successful J.E.D.I. initiative. Over the long-term, perhaps far more than $22 million worth of benefit, if such a thing could be calculated. So, if strong evidence emerged that changing our name would substantially improve NSGCs odds of a successful J.E.D.I. program, then it’s prudent to consider this option with an open mind. We can’t just say that we’ll implement a J.E.D.I. program “unless it’s challenging or expensive,” right? If NSGCs J.E.D.I. initiative is a priority, then we should prioritize it. And maybe, there isn’t as much sacrifice as the “pro same” side implies.
Let’s also assess the state licensure argument more closely. There are lots of state licenses for all sorts of fields (see here and here for more info). Millions of people have state licenses all over the United States, including licenses for athletic trainers, auctioneers, and barbers, to name a few. So as a political matter, getting a state government to issue a professional license is often a manageable process. That’s why NSGC has approximately 35 state licenses. Importantly, a name change is drastically easier to navigate through a legislative body than a whole new license. Legislative bodies often use a “consent agenda” to take care of matters that are considered “technical and non-controversial.” It’s hard to imagine a piece of legislation that is more “technical and non-controversial” than changing the name on the genetic counselor license, as long as we don’t trigger a turf war by calling ourselves something like “doctor” or “geneticist.” In some states, we might even be able to get a name change done with volunteers, no lobbyists needed. And even in the states where we would need lobbyists and perhaps the consent agenda isn’t an option, this should not represent particularly expensive lobbying. If we genetic counselors decided to change our name, it would indeed require volunteer work to amend our state licenses, and it would have associated financial costs, but this is hardly an insurmountable hurdle – and one well worth jumping over to accomplish NSGCs Justice, Equity, Diversity, and Inclusion goals.
Next, let’s investigate the argument that a name change could hamper our efforts on Medicare recognition. Medicare is a massive and expensive federal program, and while there are different ways to calculate it, many legislators believe that recognizing a new provider, such as a genetic counselor, would represent a cost to a program that is already too expensive. So, unlike a state license, getting the United States Congress to recognize a new provider under Medicare is politically extremely difficult. In fact, after nearly two decades of effort, NSGC still hasn’t made any substantial progress on Medicare recognition, which in the context of this debate (and really only in the context of this debate), is actually a good thing. We haven’t even made it through the House or Senate. So, our lack of Medicare recognition at the present time argues in favor of exploring a name change, not the other way around, since our bill is still going through a process where amendments are common anyway.
To summarize, the benefits and costs of changing the genetic counselor title have not yet been fully flushed out. The debate at NSGC, while very thought provoking, was a starting-off point. We need to identify the best contender for an alternate name, and assess the benefits the alternate name is likely to generate. Perhaps the right name could both bolster the J.E.D.I. action plan and improve our prospects of gaining Medicare recognition, by better succinctly representing a genetic counselor’s value to the healthcare system. In parallel, we need to understand what the costs would be specifically for genetic counselors, as opposed to using Physician Assistants (I mean, Associates) as a proxy. PAs can already bill Medicare, have a different scope of practice, there are about 150 thousand of them in the United States, and there are likely many other differences. While their experience is of course informative, they are not a reasonable proxy. Once we have a better sense of what a name change would mean specifically for genetic counselors, then we can weigh the estimated benefits of the identified new name against the estimated costs. Importantly, when assessing the costs, we shouldn’t only ask lobbyists who expect to bill us for their services, as they have an obvious financial conflict of interest.
A successful J.E.D.I. program was always going to require substantial work, cost money, require new ideas, and require openness to meaningful change. Changing the genetic counselor name would indeed require NSGCs political operation to put in effort, but what is the point of having a political operation if we’re afraid to interface with the political system? If we can’t identify a new name that would propel NSGC’s J.E.D.I program, then it’s not worth the cost and effort. But I strongly support researching a new name further, and politically speaking, if we can’t handle a name change to a state license, then we can’t handle much of anything. And a name change may be easier than Mr. Resta’s charming idea that we convince George Clooney and a major network to launch a TV show about genetic counselors that’s as successful as the Sopranos.
There’s a lot of tricky questions that arise that aren’t touched on in this piece. A name change would need to be a slow and thoughtfully planned process – staffing, volunteers, timing, budgets, and not to mention the new name itself. There are likely other costs that haven’t been identified yet. We might not even like the new name, but remember, it’s not for the majority of current genetic counselors – it’s for the future of genetic counseling.
Misha Rashkin has been a genetic counselor for 10 years. He is a clinician and specializes in oncology. He has a longstanding interest in the ethical and legal issues of genetic testing, particularly the Genetic Information Non-discrimination Act (GINA).
At the recent NSGC Annual Conference, Carla McGruder chaired a sparkling plenary session titled “Say My Name, Say My Name”during which panelists debated the pros and cons of the professional title Genetic Counselor (there was widespread disappointment that Beyoncé did not make a guest appearance). The general sense I got from the debate was that there was enthusiasm for a name change and that a new professional title may ultimately prove to be destiny’s child, but for now no one offered a particularly winning alternative (see below word cloud from the session). Perhaps unsurprisingly, nobody brought up my two biggest long-standing concerns about the genetic counselor title. One is that the oft-used abbreviation of GC for genetic counselor is also the abbreviation used for gonococcus bacteria (though then again it could also more appropriately suggest guanine and cytosine). My other concern is that we should more properly be called genetics counselors; genetic counselor without the “s” at the end of genetic makes it sound like being a counselor is a hereditary condition, the result of some likely pathologic variant. I am pretty sure, too, that lots of genetic counselors in Canada, the UK, Australia, and some other countries would prefer everyone spell it “genetic counsellor.”
Word Cloud for suggested alternative professional titles for genetic counselors, from “Say My Name, Say My Name” panel discussion at the NSGC’s 42nd Annual Conference in Chicago, October 20, 2023. Reproduced with kind permission of session chair Carla McGruder, MS, CGC.
Debate about what to call ourselves has surfaced with some regularity since the profession was birthed a half-century ago at Sarah Lawrence College, and in a journal article by Jehannine Austin and their group at the University of British Columbia, as well as being the subject of two prior DNA Exchange postings, one by my DNA Exchange colleague Allie Janson Hazell and one by me. I suspect that currently the name debate is driven by the profession’s expansion into so many new employment niches, many of which do not involve direct patient care. It may also be influenced by the increasing trend of the profession defining itself – and being defined by other health professionals – in relation to genetic testing.
Let me state my biases up front. I am opposed to a name change, at least until you can show me something better that will justify the very extensive, expensive, and intensive efforts of introducing a new name and eliminating an old one. Of course, my biases are partially driven by being an Old School GC, having graduated in the Late Neolithic Period of genetic counseling, back in 1983. There’s always the attitude of “Damn it, the way I was taught is the right way.” And even if someone comes up with a better job title, I will still likely go to my grave calling myself a genetic counselor. But my personal hang-ups and emotional reactions aside, let’s take a look at some of the pro arguments and why I think they fall short.
One of the pro arguments for a name change centers on lack of public awareness of just what a genetic counselor is or does. Yeah don’t we all know that one! I can’t disagree with this point. But changing our name will not in and of itself improve public awareness or visibility. The alternative names are equally or more ambiguous. Patients will probably react with uncertainty to titles that include the likes of analyst or consultant or specialist (to name just three) and it will do nothing to clarify how we might help and serve them.
While acknowledging the general lack of public knowledge about genetic counselors, we have nonetheless made remarkable progress in increasing awareness of the job title, both with patients and healthcare providers. The below Google Ngram, with all of its limitations, gives a rough idea of how much awareness of genetic counselors has increased since Sheldon Reed christened us in the 1940s, with the ambiguous but reasonably accurate definition of “a kind of genetic social work.” A lot of that progress can get lost if you eliminate the genetic counselor title.
If you really want to improve public awareness, you have to think beyond name changes and PR campaigns. Look at what the Dr. Jennifer Melfi character in The Sopranos did for publicity for therapists. What we need is a successful streaming series about genetic counselors, complete with gratuitous sex and nudity (we can hold off on the violence; there’s more than enough of that to go around in the world these days). I can picture the genetic counseling show’s log line: “Family Lines” – Follow the professional challenges, joys, tragedies, and dilemmas as well as the complicated personal lives of young, attractive, ethnically and gender-diverse genetic counselors as they graduate from their training programs and experience the impact of genetic conditions on their patient’s lives and families as well as on the counselors’ own psyches. Starring George Clooney as the dashing veteran Robert “Bob” Resta whose efforts to guide this gaggle of counselors throughout their careers are undermined by his own very human failings.Consider running the credits over a background of a pedigree being drawn to highlight the commonly used genetic counseling tool and to evoke the name of the show.
Proponents of a name change quite rightly claim that the term “counselor” doesn’t reflect what many genetic counselors actually do in their day-to-day work. Genetic Counselor does not capture the essence of a Variant Analyst, Professional Support Specialist, Product Development Manager, Program Administrator, Researcher, or Medical Science Liaison. But, according to the 2023 NSGC Professional Status Survey, 71% of genetic counselors are involved with full or part-time direct patient care. This suggests that a significant majority of us are actively engaged in genetic counseling on a regular basis, so it makes sense to call us genetic counselors.
Besides, the proposed alternatives capture an even smaller range of what genetic counselors do for a living or otherwise sell our skill set short. For example, one of the suggested alternatives is something along the lines of Genetic or Genomic Information Specialist. It strikes me that the word “Information” misses a critical insight into the human psyche. It isn’t so much the information that’s communicated that is key as it is the way that each person’s mind uniquely interprets that information and integrates it into their lives. this is where counseling skills come in, which, for my money, is what sets the profession apart and makes it uniquely valuable. It gives us a professional identity unlike any other genetics profession or specialty. The value of counseling and communication skills is acknowledged by many genetic counselors employed in non-direct patient care positions, who often claim that their counseling and communication skills have been key in enabling them to expand into their new roles. They are still using basic genetic counseling skills, just in a different context.
Furthermore, I would argue that the very ambiguity inherent in the genetic counseling title is what has allowed us to grow our professional roles. Other professional titles might not provide the flexibility to expand into new and exciting roles. If employers are not exactly sure of what we do, it allows us create new roles that other providers don’t have the knowledge base or skill set to match. As Ed Kloza – who has pretty much witnessed the entire history of the profession first hand – sagely pointed out at the microphone at the “Say My Name, Say My Name” session, the title genetic counselor has gotten us pretty far professionally since the 1970s. Just how has it limited us?
A decidedly practical drawback to changing our professional title lies in the bureaucratic underpinnings necessary to maintain the life of a profession. It’s not just a name that can simply be eliminated by a search-and-replace function. The title Genetic Counselor is written into state licensure laws, pending federal legislation to make genetic counselors recognized Medicare providers in the US, and other countries’ equivalents of licensure. To say nothing of changing job titles by every employer of genetic counselors, the names of a half dozen or so professional organizations, a journal title, and a PubMed search term, to name a few. This could potentially be achieved but you need a very, very compelling reason to expend all that energy, time, and money doing so.
It will be interesting to see what what happens with the job title in countries where the genetic counseling profession is just establishing itself – such as India, the Philippines, and the Middle East. Local circumstances, medical practice, and cultural preferences may wind up generating some very different names and professional practices. But I suspect that they may also want to stick with the genetic counselor title to capitalize on the remarkable progress the profession has made in the US, the UK, Canada, Australia, and elsewhere. The practice and profession may look a bit different around the globe, but they will still be recognizable as genetic counselors and not as something else.
Perhaps too, it is time to reconsider the 2006 standard definition of genetic counseling. While I happen to be a champion of that definition, my professional conflict of interest is that I helped craft it. The current generation of genetic counselors should not necessarily have to rely on a definition created by a previous generation if it no longer captures the essence of genetic counseling. This could have bearing on whether we should choose a new professional title.
For now, though, Genetic Counselor may be a less than perfect name but it is closer to perfect than the proposed alternatives. Give me powerful reasons to think otherwise, and I will change my mind. Until then – Change my name? Nah.
My professional life up till this point has been centered around a mission to bring genetic counseling to people who – like me – live with psychiatric conditions, and their families. This has been my mission for >20 years, since my family started asking me about whether psychiatric conditions were genetic and what this meant for us while I was doing my PhD on this topic. Realizing that it wasn’t just my family that had these questions and that no-one was really addressing them is what drove me to train as a genetic counselor. Once I completed my genetic counseling training in 2003, no one would hire me to provide genetic counseling for families with psychiatric conditions. Of course, psychiatric conditions have always been profoundly disenfranchised in terms of health services, but as well, there was no evidence that people with psychiatric conditions wanted genetic counseling, and no evidence that it could help. So, this drove me into research.
I landed a research professorship and my team and I generated data showing that:
people with psychiatric conditions wanted access to genetic counseling
genetic counseling helps people with psychiatric conditions
In 2012, on the strength of these data, we established the Adapt clinic – the world’s first specialist psychiatric genetic counseling clinic. It was all about helping people understand the factors that contribute to developing a psychiatric condition, and how to use this understanding to engage in self-management strategies to protect their mental health for the future. It was about helping people to make meaning, and understand that psychiatric illness is not your fault, and not your fate.
In 2023, after 11 years of helping patients, training students, generating research data about the impact of what we do, and providing a model for psychiatric genetic counseling services around the world, our service is being closed.
I’ve fought this with everything I have because it feels so wrong. But I’m so bone tired …and there’s literally nothing more I can do. It’s over.
No amount of data demonstrating the awesome outcomes that patients experience (increases in empowerment, changes in behavior to engage in self-management strategies to protect their mental health) after receiving our services has swayed the decision. So, this is a eulogy.
The webpage for the clinic has silently ceased to exist.
The reason given for the death of the Adapt clinic? To redeploy the counselors to provide service for general genetics patients because the waitlist there is so long. It’s apparently that simple. And pointing out that this is classic disenfranchisement of people with psychiatric conditions – again, people like me – has made no impact. I may as well be speaking to a wall.
Now, as someone who has served as a leader myself in a publicly funded healthcare setting, I do of course understand that we are forced to make decisions about how to allocate scant resources. And sometimes people might not like the choices we make. I understand that. My objection is that the Adapt clinic embodies (has embodied) all of the principles and values claimed to be held dear by the healthcare system that is closing it. That is what I find distressing.
Initially, when I saw the writing on the wall that the clinic would be closed, I was devastated- this was my life’s work, I thought. And it’s been for nothing, my internal voice said…I am a failure. I lost all energy to continue in my efforts to leave things better in the world than I had found them. Because, what is the point? I – and the counselors within it – gave the Adapt clinic everything we had, it was demonstrably successful, and yet it is still being closed….it felt like it was all for nothing.
But this narrative is wrong. I can see that I am not a failure, and that the clinic was not a failure. Instead, the clinic, and the counselors within it, and the patients we serve, have all been failed by the system we are in.
Our efforts were not for nothing. The Adapt clinic has helped about 1400 patients and trained over 50 students, some focused on clinical skills, some focused on research skills, and some both. We published about 20 papers that are out there in the world that explain the difference that psychiatric genetic counseling can make for people, and how to do it well. I know that we have inspired practicing genetic counselors around the world as well as students…we have inspired people to train in this discipline. I know this because people have been gracious enough to tell me about how our work has affected them.
Given all this, you have to ask, why is the clinic dead? I think there are two real answers to that. First, psychiatric conditions are still so stigmatized. People with mental illness – like me – have a long and awful history of being disenfranchised, and here we see it again: an evidence-based service for people with psychiatric conditions cut, despite data showing that it’s needed and it helps. And yet it’s cut so that we can prioritize providing services for people with non-psychiatric indications.
Second, the genetic counseling services we provide for people with psychiatric conditions typically don’t involve genetic testing. And though the service helps people, the health system decision-makers don’t value genetic counseling when there’s no genetic testing being done. The psychotherapeutic work we do is not valued …which is truly the hardest thing for me to swallow, because data show that it’s exactly this that makes the difference even when genetic testing *is* available. It’s the counseling that helps people.
So, yes, this is a eulogy — a public expression of pain and grief and disillusionment about the death of a clinic whose establishment was the culmination of >10 years of my work, that we nurtured successfully for 11 years, and that brought purpose to my life and a way to channel my own experience of psychiatric illness to help others. It’s so hard to build and create something new and innovative, and so very easy to destroy it. It does feel like a death.
My biggest fear is that others will stop trying to establish psychiatric genetic counseling clinics in other jurisdictions as a result of this. People – like me- who have psychiatric conditions deserve better than this. So please keep pushing. Others have taken up the mantle – there’s a clinic in Cardiff, and Tennessee, and others (if you know of others, please tell me!)… I’m rooting for all of you. Please let me know how I can help.
But I think this reflects broader issues too – I think as a profession, we have to answer some questions for ourselves. Are we happy with being reduced to roles as the purveyors of genetic testing? And only post-test counseling at that? This is the direction in which we are headed. Medical genetics departments with long and growing waitlists often respond by simply reducing the list of indications to make fewer people eligible to access genetics services. That’s exactly what happened to the Adapt clinic — the eligibility criteria for access to genetics services shrank to exclude our patients. What happens to these patients? It’s not that they get service elsewhere – they don’t. The people who make these decisions are deciding who gets care — deciding who matters. This is an issue that relates to equity and justice.
In writing this eulogy for the clinic that I created and loved, my purpose is to try to use its death for something positive. Given our increasing focus on the importance of EDI issues, I would like to suggest that this is an opportunity to question whether tertiary-care clinical genetics is the right location for genetic counselors if we are to be able to provide just and equitable access to our services for people who need them. Situating genetic counseling services in alternative locations, such as primary care/family practice, might be worth considering as a way to ensure our ability to practice to the top of our scope, to offer more than just genetic testing (like psychiatric genetic counseling), and to ensure more equitable access for patients.
I hope that the end of Adapt can be used as an impetus for the start of something new. If the Adapt clinic has impacted you in some way, those of us who nurtured it would love to hear about it in the replies, or by message.
Some of my fave quotes from people who had psychiatric genetic counseling in the Adapt clinic (from Semaka et al 2019):
“Until genetic counseling, no one ever coherently explained to me why I have a mental illness. And I think that’s a conversation that needs to be had because most people just think they’re having a bad time of it or they just think that they just need to try harder”
“I felt in control, you know [psychiatric genetic counseling] made me feel more empowered than I did when I walked in and I think for me that’s a big deal… I just felt after the appointment I had more tools to control my life.”
“[Psychiatric genetic counseling] gets rid of some of the shame…. with mental illness, it’s so hard to know what you did wrong but really you didn’t do anything wrong and [psychiatric genetic counseling] just explains that to you… so you’re able to look at this and think, ‘OK, this isn’t my fault’”.
Justin Lorentz is a certified genetic counselor who graduated from McGill University in 2012. He spent 8 years working in cancer genetics at Sunnybrook Hospital in Toronto, Canada where he developed an academic interest in prostate cancer genetics. He now works at Sunnybrook one day a week leading their Familial Prostate Cancer Clinic. Justin spends the rest of his time at Medcan, a Canadian preventive healthcare clinic offering proactive genetic testing, pharmacogenomic testing, carrier screening, NIPT, and healthy whole genome sequencing.
Two years ago, I saw the NSGC rebrand a pillar acronym for DEI initiatives into a pillar franchise: Star Wars, and more specifically, their JEDI. This was at a time when J for Justice was starting to be included in many Diversity, Equity, and Inclusion (DEI) committees. Most committees threw the J on the end. The NSGC did not, and on April 8th, 2021, the NSGC released an introduction to the J.E.D.I. Committee. The potential of the Star Wars franchise reference to trivialize the efforts of the committee was brought up in the publication, but the post argued JEDI is easier to say and through “listening and conversation with others” a vote was struck up with the committee to settle on their name: the J.E.D.I Committee.
And the NSGC was not alone. The American Association of Geographers, Big Brothers and Big Sisters of America, heck, The Canadian Psychological Association all have a JEDI, and many JEDI committees lean into it, lightsabers, and all.
But something about the J.E.D.I. acronym never sat right with me. I remember thinking, imagine if the letters DEIJ magically spelled out MUGGLE, and the NSGC’s DEIJ committee adopted the M.U.G.G.L.E acronym instead. What would happen to that committee’s name after J.K. Rowling would go on to make her TERFY statements on trans women? Rebranding DEIJ to a franchise is risky because you have no control over how that franchise’s brand can evolve. It’s begging for a PR problem. But even more so, what do Harry Potter and Muggles have to do with DEIJ or genetic counseling? If the answer is nothing, then the risk of rebranding DEIJ into something it isn’t is not worth it to me.
Over the years of seeing the J.E.D.I. acronym on NSGC updates in my Gmail inbox and on Twitter, my thoughts on the J.E.D.I. acronym for a DEIJ initiative started maturing. I debated whether my issues were worth publicly expressing until I came across this Scientific American article which summed up my growing concerns, and more.
After dwelling long enough I decided my need to express my opinion more loudly. I agree with the NSGC DEIJ Committee’s initial instincts that the J.E.D.I. acronym does trivialize the DEIJ Committee, but to me that just scratches the surface. When you dig but a little deeper, you realize that JEDI has its own meaning, a controversial history, and a diehard fan base. It not only distracts from DEIJ work, but I think the word JEDI opposes DEIJ work, not just for our professional organization, but for any organization.
There’s a lot to think about and you need to know about the Star Wars franchise to really put it all together. I realized this as I ran this DNA Exchange blog post by my partner, who has never seen media from the Star Wars franchise. Although it’s probably safe to assume most people attuned to Western culture know what a Jedi is, the more you learn about Jedi and their Order, the more problematic it all becomes as the title for any DEIJ work.
In case you’re someone who does not feel included in my previous assumption that most folks know what a Jedi is, let me sample Merriam-Webster to do the definition justice, so we’re on an equal playing field. *Nerd mode activated* Jedi are a very select group of monk-like galactic warrior/priests, both humans (the historic stars are white cis-gender males) and alien (Yoda), who are proficient with melee weapons called lightsabers. They’re all born with a seemingly inherited wealth of abilities including accessing and manipulating a spiritual/cosmic energy called The Force to perform supernatural feats like levitation and the famous Jedi mind trick (Eek! There’s NSGC J.E.D.I. Action Plan Task Force – How many other communications from the J.E.D.I. committee could/have become unintentionally conflated with trivializing aspects of the Star Wars franchise?).
Jediism, like Scientology, has made its way from the sci-fi world into the real world. In 2005 the Temple of the Jedi Order was registered in Texas and was granted federal income tax exemption by the IRS in 2015. The Church of Jediism purportedly boasts up to 500,000 members worldwide. Although faith is an important part of a patient’s values and decision making, the genetic counseling profession is not aligned or defined by any one faith, especially not this one. It’s a bit out there, but the NSGC’s J.E.D.I. Committee is sharing a brand with Jediism, even if it is in name only.
Let’s explore the idea of a PR problem further – what happens when the Star Wars franchise comes under scrutiny? More importantly, what if the scrutiny is DEIJ related?
Law and Philosophy professor Patricia Williams wrote a very compelling article called Racial Ventriloquism in 1999 after Episode I: The Phantom Menace came out. Here she highlights racist depictions of two alien characters from the Star Wars franchise: one popular, one more forgettable (until now).
Exhibit A) Jar Jar Binks: He’s a Gungan, an amphibious alien species with a frog-like face. He’s portrayed a little less clever than the average alien, panicky, having poor judgement, and being clumsy. He is the main source of comic relief and he and his species share a characteristic jovial, swaying saunter complete with a striking West African, Caribbean, and African American linguistic style. Patricia quotes a few phrases here to jog your memory if you haven’t heard him talk in a while: “You-sa Jedi not all you-sa cracked up to be.” “Me berry berry scay-yud.” “We-sa goin in da wah-tah, okeyday?”.
Exhibit B) Watto: He’s a Toydarian, a potbellied alien with insect like wings and a large nose like a tapir. He’s portrayed as a money-obsessed junk dealer and slaver. His accent seems Middle Eastern, and Patricia notes he bears eerie resemblance in shape and clothing to a cartoon published in Austria’s antisemitic Kikeriki magazine, right down to the hat.
These are two examples of many controversial aspects of the Star Wars franchise brought up over the twenty-four years since the release of Star Wars: Episode I – The Phantom Menace. Admittedly I forgot aspects of these controversies and it took researching them to realize the incredible depth of the problem. I’ll be honest, I wouldn’t expect anyone to be digging into the racial allusions the Star Wars franchise had made over 20 years ago when considering using J.E.D.I. in 2021, but now that we’re here I think we can all agree it’s hard to unsee.
And what about now? It’s not only the Star Wars franchise that’s racially controversial, but also some of its fanbase. Take the more recent racist backlash of Star Wars fans when the now Disney+ owned Star Wars franchise introduced Moses Ingram, a Black female Sith-like antagonist in the Obi-Wan Kenobi series released last year in 2022. Unfortunately, she’s not alone; other actors have faced similar racist attacks:
Ahmed Best (Black actor who played Jar Jar Binks) that was so persistent he contemplated suicide
Kelly Marie Tran (Asian actor who played Rose Tico) in The Last Jedi and The Rise of Skywalker
It’s debatable whether this reflects poorly on the Star Wars franchise per se, but what it does show is the franchise attracted fans who expect something of the franchise, fans who have their own preconceived beliefs of what they want lead characters in this Jedi series to look like.
How are we feeling after all of this? What are you thinking about right now? Are you seeing the word Jedi through a different lens?
I am.
For me, Jedi, and the Star Wars franchise that birthed Jedi, do not have a place in any DEIJ committee due to Star Wars’ bizarre religious movement, racial controversies, and certain members of their fanbase with strong opinions on the diverse direction the franchise is trying to tale. The word Jedi carries a lot of its own baggage and its own meaning.
To me, DEIJ means what it is: Diversity, Equity, Inclusion, Justice. It may not be easy to say, but neither is 2SLGBTQ+, and neither is challenging our own internal biases ingrained in us from a society built on systemic racism, sexism, ableism, and other injustices. Let’s keep DEIJ as its own important and well-established brand.
The initial reasoning for the NSGC DEIJ Committee to be called J.E.D.I. was fair for that time, and the NSGC’s newly forming DEI committee was not alone in their thought process. Knowing more at this time, I don’t think the NSGC’s J.E.D.I. Committee should continue calling itself something it isn’t. I hope the work of any DEIJ committee is nothing like the work of the Star Wars franchise or their Jedi. In fact, I feel Jedi go against DEIJ committee work. I want to see every DEIJ Committee for what it is, a hard to say acronym, making hard to do changes in what I think is one of the most important areas of development in our profession over the next few years. I think it’s time for a rebrand.
These are my thoughts – I’m interested to hear yours.
Ka mua ka muri (Walk backwards into the future with your eyes fixed on the past) – Maori whakatauki (proverb)
The NSGC Pedigree Standardization Task Force, of which I am a member, recently published updated guidelines for pedigrees, with a focus on sex and gender inclusivity.* Essentially, the guidelines state that the symbolic representation of individuals in a pedigree should be based on self-identified gender rather than sex assigned at birth. Squares, circles, and diamonds for people who identify as men, women, and non-binary people, respectively, supplemented by clarifying annotation when appropriate. A subtle implication of gender-focused pedigrees is that the internal logic of pedigree construction is no longer compatible with exclusively placing the “man’s family on the left and the woman’s family on the right” (to use the gendered language of yesteryear; more gender neutral but more awkward sounding terms might be sperm provider and egg provider). This point was illustrated in the article’s accompanying tables but not specifically called out in the text, though it is the subject of a brief follow-up Commentary. Of course, the discretion of which side of the pedigree to use for which side of the family is up to the individual counselor’s preference. It may take some getting used to, especially for those of us who have been drawing pedigrees for a very long time (“Oh no, how am I ever going to spot x-linked inheritance?”). But it’s a freeing choice rather than a restrictive mandate.
The reasons behind abandoning the long standing left/right tradition is straight forward. If pedigrees are based on gender, there are more than 2 genders, so a pedigree cannot logically and consistently be divided into halves. For example, if you are working with a couple in which one member was assigned male at birth but identifies as a woman and the other assigned female at birth but identifies as a man and has undergone gender-affirming surgery, which person goes on which side of the pedigree? Furthermore, gender identity may change over time and so placing an individual’s family lineage on the left or the right based on gender could result in the unnecessary and confusing re-drawing of pedigrees over time. Eliminating the left/right prescription also de-prioritizes males, who previously would be the first person encountered when “reading” a pedigree from left to right. Yes, I recognize that a pedigree can be read in many ways, not just left to right, and the proband arrow is the initial focal point that draws you into the image. But the standard reading frame in Western languages is left to right. And the pedigree’s generation/individual numbering system (I-1, I-2, II-2, etc.) is such that individual #1 in the pedigree (I-1) is usually the male founder of the paternal lineage.
Pedigrees and genealogies in one form or another go back well over a thousand years. During that time, while it has been by no means uniform and universal, the majority of pedigrees followed the paternal lineage left/maternal lineage right tradition. So how did this tradition arise (for clarity, I’m going to stick with the terms paternal and maternal to keep with the linguistic flavor of the times during which pedigrees have evolved)? One possibility, of course, is that it was a fifty/fifty kind of thing. When you divide the world up into two genders, one gender’s family will wind up on the left and one will wind up on the right and so it may have been that the paternal lineage just wound up on the left and the maternal lineage wound up on the right. But I think that a trip back through the history of pedigrees and other genealogical diagrams reveals the influence of the Western male gaze in establishing this tradition, along with eugenics, and, of all things, the Roman Catholic Church.
Let’s start this backwards journey in 1995, when the Pedigree Standardization Task Force published it’s original guidelines. Figure 2 in that article states “If possible, male partner should be to left of female partner on the relationship line.” Why did we make that recommendation? Because, well, that’s the way we were taught to draw pedigrees. It was a given; we didn’t think about it too much.
Go back about a century or so, and we see the role of eugenics in shaping pedigree format. In 1912, the Eugenics Record Office (ERO) published Bulletin No, 7, The Family History Book. Page 94 of that booklet contains a somewhat condescending critique of a pedigree of a “dysgenic” family, drawn by one the ERO’s primarily female Eugenic Field Workers, for the purposes of illustrating pedigree standards. The authors state “In this pedigree, the field worker has charted the males to the right and females to the left; this should be reversed for sake of uniformity of practice.” But they make no mention of where/why that practice arose. This same ERO publication recommended using the generation/individual Roman/Arabic numbering system for generations and individuals alluded to above.
Over in England, the male gaze was at work as well. The Treasury of Human Inheritance, a key publication in the history of medical genetics and eugenics and first published in England in 1912, recommended using the Mars symbol (♂), the archetypal manly God of War, to depict males and the Venus symbol (♀), the archetypal female Goddess of Love, to depict females. Francis Galton’s book Natural Inheritance, published in 1889, contains what he describes as a schedule for recording a family history in Appendix G. Not exactly a pedigree but same idea. In this schedule, “Father and his fraternity” are on the left and “Mother and her fraternity” are on the right. Galton, by the way, believed that males were inherently smarter than females.
Galton’s recommended Family Schedule, Appendix G, from his 1889 book Natural Inheritance.
Now we take a larger leap backwards in time to the 16th century and the establishment of the College of Arms, which is still active today and is the “official heraldic authority for England, Wales, Northern Ireland and much of the Commonwealth including Australia and New Zealand.” Essentially the College of Arms assigns a coat of arms to a family based primarily on family history. This institution has been collecting pedigrees for about 5 centuries, typically with the format of paternal lineage on the left/maternal lineage on the right.
Even in modern days, with a few exceptions, women are expected to display the coat of arms of either their husband or their father. If she chooses to display both, the husband’s coat of arms is displayed to the left or above the wife’s family’s coat of arms.
Another method of displaying a family history is the ahnentafel (usually translated from German as “ancestor table”). An ahnentafel lists a family history horizontally from left to right. Individuals on an ahnentafel are assigned specific numbers that cleverly allow you to determine the relationship to the proband without scanning through the entire table. The first ahnentafel was published in 1590 by the Austrian nobleman Michaël Eytzinger and it depicted the ancestry of Henry III of France. Note that the father’s lineage is above the mother’s lineage.
Ahnentafel of King Henry III of France, published in 1590 by Michaël Eytzinger, from Wikipedia.
Carolingian (i.e., from Charlemagne) Pedigree from the late 12th century. Note at the top that the ancestral king is one the left and the ancestral queen is on the right. From The Genesis of The Family Tree by Christians Klapisch-Zuber.
It may come as a surprise to some that the Roman Catholic Church, an institution steeped in patriarchy, had a hand in emphasizing the importance of pedigrees and in shaping their format. The Catholic Church was the dominant authority in medieval Europe and played a role in regulating nearly every aspect of the lives of nobles and peasants alike. Going back to at least the 7th century, the Catholic Church had strong prohibitions against consanguineous unions, what they classified as “an impediment to marriage.” The bans extended well beyond first cousins. To guide prospective mates, the Church produced an arbor consanguinitatis, a generic diagram indicating how close various relations were to a given individual, often drawn with, you guessed it, the paternal lineage on the left and maternal lineage on the right. Of course, for the right price and for the right person, the Church was willing to permit such unions, and also to annul the same marriage on the grounds of consanguinity when that became convenient. As they did for Eleanor of Aquitane’s 12th century marriage and subsequent annulment to her relative King Edward VII of France, and then overlooked it again in her subsequent marriage to very-soon-to-be King Henry II of England, another of her relatives.
Arbor consanguinitatis, from Isidore of Seville’s 7th century manuscript Etymologiae. Note that the paternal lineage is one the left and the maternal is on the right.
The Catholic Church also employed pedigrees to illustrate the genealogy of Christ, the so-called Tree of Jesse (Jesse was the father of Goliath-slaying David and a direct ancestor of Christ). This was especially useful for instructing those who could not read the Bible, which was practically everybody who was not a priest or a noble. The earliest known Tree of Jesse dates to 1086, though the tradition of graphically depicting biblical ancestry goes back at least to The Great Stemma, which is thought to date to the 5th century (The Great Stemma, like modern pedigrees, also has a left-to-right reading frame, starting with Adam). Jesse Trees typically depicted only the male ancestors of Christ, along with various other Biblical personages on the sidelines, cheering on the progression of the generations. These trees typically omitted Mary’s lineage (though often included an image of her) but did include the ancestors of Joseph, who technically is Christ’s stepfather and not his biological parent. Many include an actual tree emerging from Jesse’s groin, an image sometimes referred to as, ahem, “the rod of Jesse” (males and their delusional obsession with their penises, thinking they give rise to great trees!). It was not uncommon for kings to insert themselves into a version of a Tree of Jesse, likely in an attempt to show divine approval of their kingship, such as the elaborate family tree of England’s King Edward IV produced in 1461. The trees took on many forms over the years and can be found as illustrations in manuscripts, carvings, and on stained glass windows churches even to the modern day.
Tree of Jesse, depicted on a stained glass window from the Cathedral of Our Lady Of Chartres.
Rod of Jesse, by the Flemish engraver Johannes (Jan) Wierix (1573)
Another way that the Catholic Church may have influenced the appearance of a pedigree – and here I am speculating – is that it’s traditions may have been the source of placing the paternal lineage on the left and the maternal lineage on the right. A Catholic altar is often divided up into three parts – center, right, and left. The center is devoted to God. The right side – from the perspective of a priest looking out at the church – is devoted to Mary, the female. The left side is often devoted to Joseph, the male. Thus, think of looking at a pedigree as a priest looking out on a Church – paternal lineage to your left, maternal lineage to your right. Furthermore, in Catholic iconography, Mary is typically depicted as the right hand of Christ in Heaven. So it would be natural to follow that tradition when drawing a pedigree.
The story of the pedigree is more detailed and complex than I describe here, and probably goes even further back to the Roman Empire. What the story reveals is that even though a pedigree is an apparently objective and straight-forward graphical depiction of ancestry, it is suffused with the values of the people who construct them. The male bias in pedigrees was so embedded in Western European culture that it naturally spilled over into the architecture, appearance, and content of pedigrees. Sometimes those values are consciously articulated, as with the Task Force’s decision to recommend a gender-focused pedigree. More often, though, those values and biases are so engrained that we can’t see or perceive them, unless we march into the future with our eyes fixed on the past.
Gender-neutral language has evoked anything but neutrality. What with snide remarks about non-gendered pronouns and the politicized and contrived fears about how such language is a sinister plot to groom children for non-heterosexual behavior and non-binary gender identities, you would think gender-neutral language is a major threat to democratic institutions or an existential crisis for humanity on the scale of climate change. But these attacks lack substance and mostly just reveal a lot about our conscious and subconscious insecurities and biases, as well as our uneasiness with change. Language, especially the language of science, needs to be respectful and supportive of all people in all their infinite variety. Being decent shouldn’t be hard.
It doesn’t have to be this way. The history of the word “sibling” demonstrates how a gender-neutral term can be readily incorporated into language without fanfare or brouhaha (a word whose origin is said to be the sound of the cry – Brou-Ha-Ha! – made by a devil disguised as a priest, a stock character in French medieval plays). The story of sibling also takes an interesting detour through eugenics, craniometry, sexism, and fragile male egos.
Both sib and sibling go back to Old English around the year 1000 CE. Sibb, as it was often spelled in Ye* Olde English, simply meant any relative, regardless of gender or sex. The -ling suffix in sibling at the time likely did not have the diminutive implication it acquired later, and probably implied a sense of “familykind,” like adding -kind to human to yield humankind. Both sib and sibling mean the same thing. Incidentally, sib is cognate with the -sip ending of the word gossip, which came from the Old English word godsibb, a sponsor or godparent. Many centuries later, through the vagaries of language change, gossip developed its modern sense of petty talk about others that may or may not be true, an etymologically appropriate connection considering all the gossip about gender neutral language.
Old English had grammatical gender, just as the Romance languages do today, which makes the gender neutrality of sibling all the more notable. Grammatical gender started to disappear from English under Viking rule in what was called the Danelaw region of England in the 9th and 10th centuries. Old Norse, the language spoken by Vikings, was not a gendered language. I reckon a bunch of Vikings were not going to sit down and make a good faith effort to learn the complicated and random gender assignments of inanimate objects of a country they had just pillaged and plundered. It was just easier to drop grammatical gender altogether. When you rule a country and have a fearsome reputation, it’s much easier to accomplish that. This also demonstrates that an entire language can become more gender neutral.
By the end of the 15th century, sibling seems to have fallen into disuse. Standard etymology sources suggest it disappeared altogether until re-emerging in 1903, although Google’s Ngram viewer indicates the word began to be used again in the last half of the 17th century, albeit rarely.
So what’s so special about 1903 that sibling should suddenly re-emerge as a common word in the English language? In 2 words – genetics and its alter-ego, eugenics, both of which took root in the late 19th and early 20th centuries. Interest in familial disorders blossomed, as did the publication of pedigrees and articles that discussed family members. Looking for a shorthand way to say “brothers and sisters” when referring to the offspring of parents, an article published in 1903 titled “On the laws of inheritance in man” in the journal Biometrika, authored by Biometrika’s Editor Karl Pearson and his student/assistant Alice Lee, included this perfectly boring but linguistically notable sentence:
These will enable us, by using the formulae of simple or multiple correlation, which depend simply on linearity, to predict the probable character in any individual from a knowledge of one or more parents or brethren (“siblings,” = brothers or sisters).
There, parenthetically snuck in at the end of the sentence, Pearson and Lee resurrected and repurposed the word sibling, although without the intention of waving the banner of gender neutrality. But the point is that a gender-neutral term can be introduced into scientific discourse and eventually common discourse as well without the collapse of civilization as we know it. Pearson’s imprimatur, given his role as editor of a prestigious journal and towering reputation as an innovative mathematical statistician, probably helped with sibling’s wide acceptance. It’s also possible that earlier authors may have used the word sibling but it has so far escaped our notice. Nonetheless, the word was uncommon enough in 1903 that Pearson and Lee felt the need to define it.
Pearson and Lee are interesting stories in their own right, and here is where the story detours into eugenics, craniometry, fragile male egos, and sexism. Pearson was a key figure in the development of mathematical statistics. Most readers of this blog are familiar with the chi-squared test, the standard deviation, and the correlation statistic r, formally known as Pearson’s product-moment co-efficient, all of which are usually attributed to Pearson. As a prominent disciple of Francis Galton, he was also a dyed-in-the-wool eugenicist. Many of his statistical innovations were developed in the service of eugenics. True to eugenic form, Pearson also reportedly called sibling “a good Anglo-Saxon word.”
Alice Lee was one of the first women to earn a D. Sc. in Mathematics at University College London. At a time when women were regarded as intellectually inferior to men, her thesis set out to prove otherwise. Managing to talk her way into a meeting of the all-male Anatomical Society in Dublin in 1898, she managed to get 35 distinguished anatomists to agree to let her measure their heads. Her thesis compared those measurements to the head measurements of male faculty at University College and to the head measurements of female students at Bedford College where she was a faculty member (Bedford College was England’s first all-female institute of higher learning). Not only did her results show no correlation between intelligence and head size, some leading anatomists and one of the men on her thesis committee had some of the smallest head sizes (talk about an intimidatingly scary thesis defense – publicly telling a committee member he has a small brain!). One anatomist had a skull capacity that was less than 50% of the women students. Her findings, as you might guess, were not well received. Her work was criticized by her committee as “unscientific” because, well, everybody knows that women’s brains are smaller and they have lower intelligence than men and the committee didn’t like having a finger stuck in the eye of their male egos. Even Galton, who was not on her committee, was asked to weigh in and he too criticized her work on the same grounds. But Lee persisted, and with support from Pearson, who backed her analysis, she was awarded her doctorate. Lee’s research, with her listed as first author, was eventually published in The Philosophical Transactions of the Royal Society. Despite her skills, she remained a low-paid assistant for her entire career and was only awarded a pension when Pearson again stepped in on her behalf.
Lee’s measurements of the brains of anatomists. Note that her thesis committee member, Sir William Turner, has the 8th smallest brain. (Image from Wikipedia)
Alice Lee, statistician, shrinker of male brains and male egos. (Image from Wikipedia)
Now back to the sibling story. English, of course, is not the only language that has a gender-neutral word for siblings. For example, German geschwister essentially translates as sibling. As does the Turkish word kardeş, which has a delightful etymology. The word was initially karindaş, a combination of karin (“belly”) + daş (“sharer”). Siblings shared a womb (usually asynchronously) and were therefore “belly sharers.”
Sibling has produced its own linguistic offspring (another gender neutral term that goes back to Old English). Nibling, a term for the children of your siblings (niece/nephew+sibling), was supposedly coined by the Yale linguist Samuel E. Martin in 1951, with a colleague “Dr. Sane.” But I have been unable to track down a citation by Martin proving this nor could I dig up anything about “Dr. Sane.” Chibling (children of my siblings) is a more recent variant of nibling. Pibling, a term for aunts and uncles (parent+sibling) was, as far as I can tell, coined in a brief 2005 article in the British Journal of General Practice authored by Dr. Neville Goodman. Perhaps I will be proved wrong, but to my ear these words sound too cute and contrived to gain wide acceptance. For what it’s worth, my spellchecker tried to correct chibling and pibling, but not nibling.
English, and many other languages, have plenty of gender-neutral terms. Introducing new terms, resurrecting old ones, or just using words we’ve always used, doesn’t need to create social drama or political warfare. No grammar drama is necessary. Language changes and the world still manages to stay on its axis.
*- For the language nerds out there, the “Y” in Ye is actually not the letter Y. It is an approximation of the now-defunct English alphabet letter thorn (Þ). Thorn is a phoneme sometimes pronounced like the th sound in “the” and sometimes like the th sound in “thick.” Thorn originated in the runic alphabet and was used in Old and Middle English. The printing press was imported into England in the 1470’s from Belgium and the Netherlands, countries whose native alphabets did not include thorn. The closest approximation that the printer’s types had to thorn was the letter y. So Ye Olde English is actually “The Old English.”


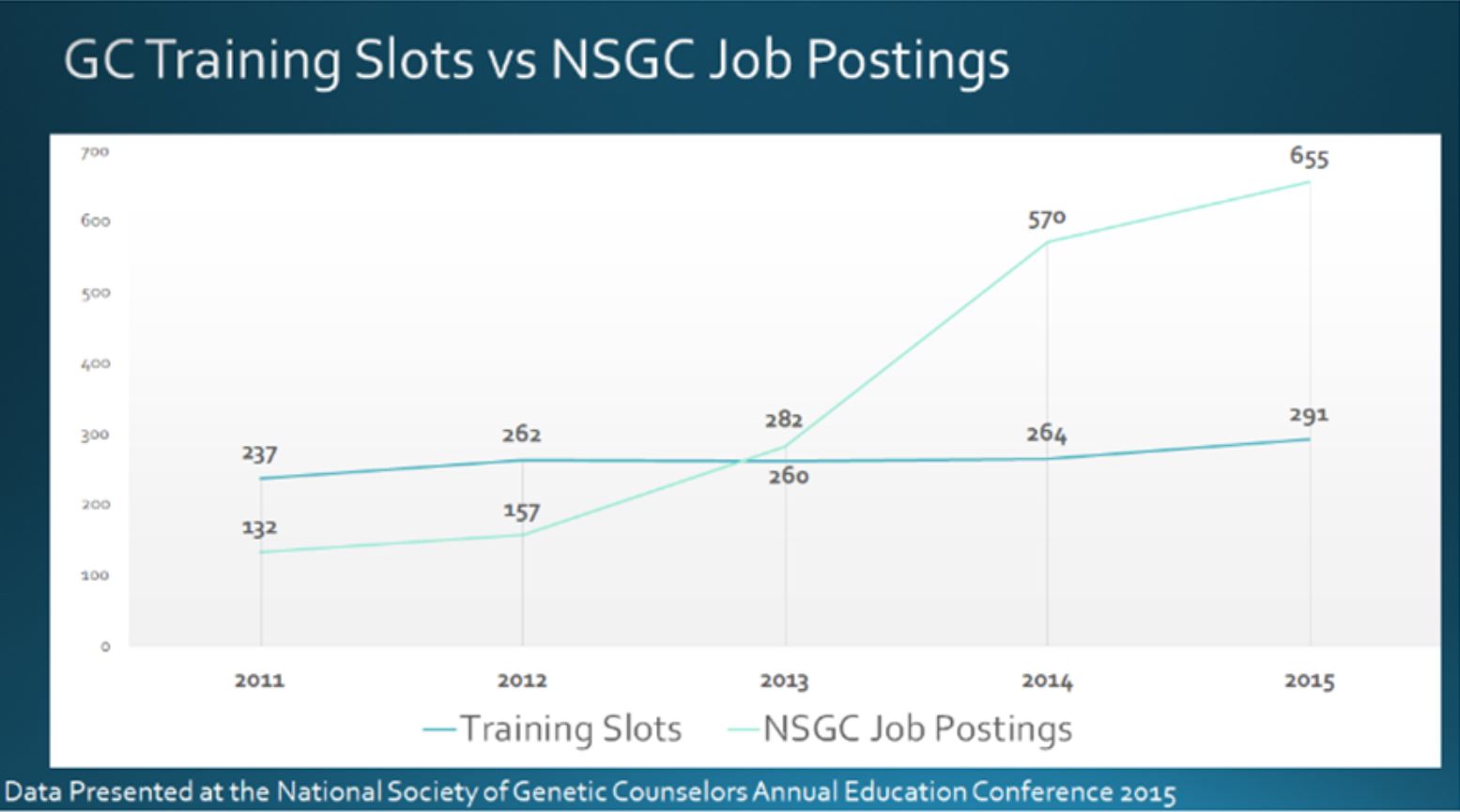






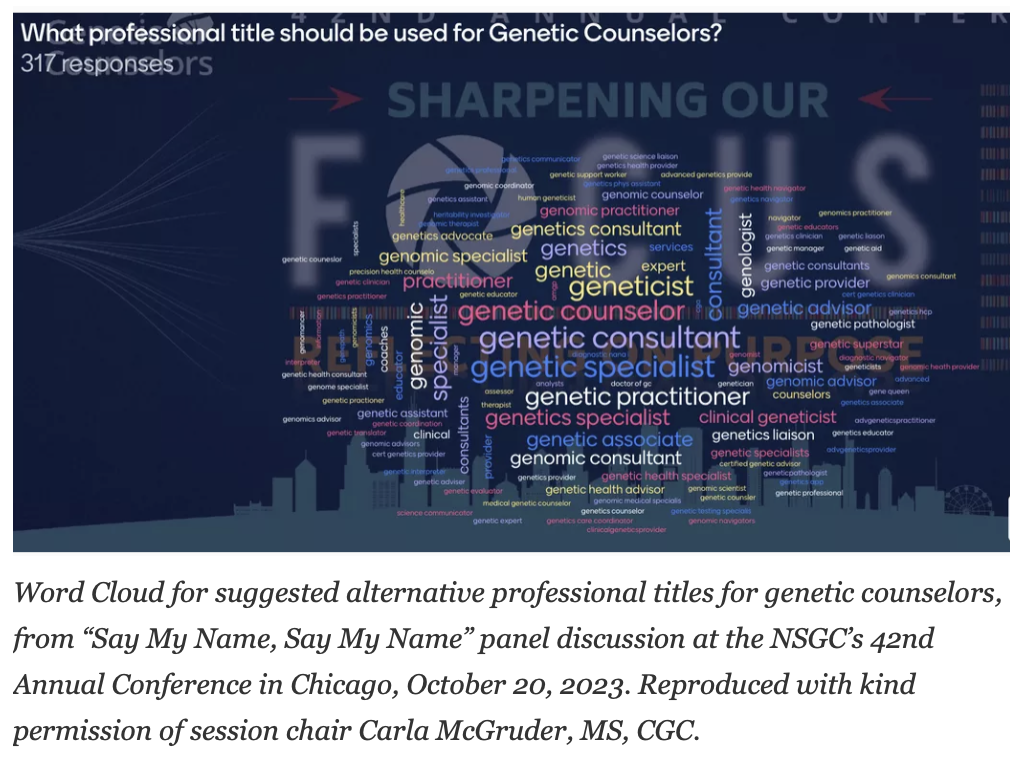






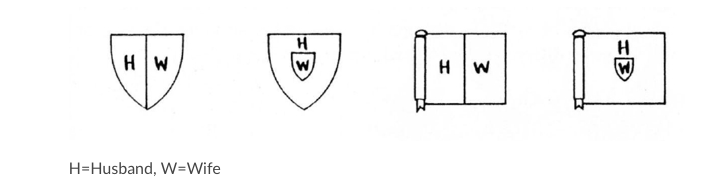

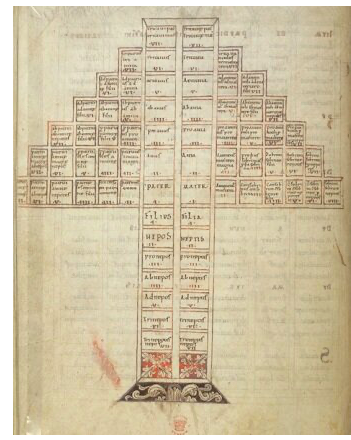



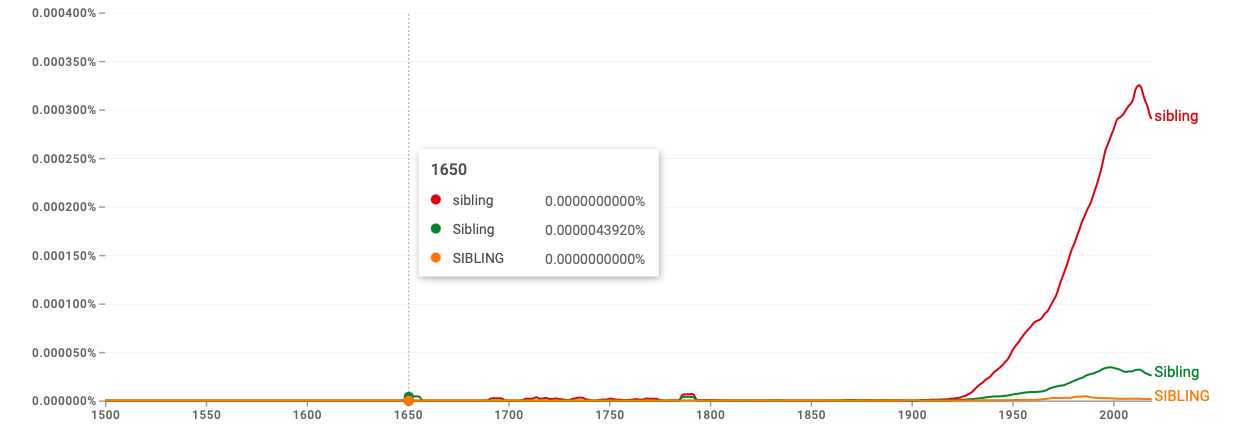
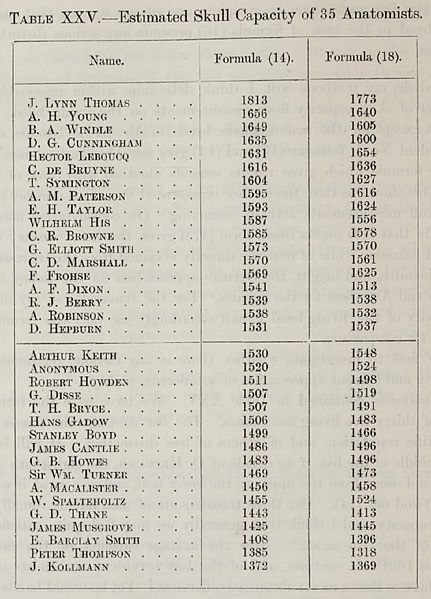


{kind=link}